Вам также может понравиться
- Miscarriage Early Pregnancy LossДокумент10 страницMiscarriage Early Pregnancy LossiwennieОценок пока нет
- Ivanaesthetics 160916154203Документ70 страницIvanaesthetics 160916154203iwennieОценок пока нет
- Osce Ear Nose N Telinga. P Throat!-From Siti Zarina. MueheheДокумент43 страницыOsce Ear Nose N Telinga. P Throat!-From Siti Zarina. MueheheiwennieОценок пока нет
- Mcqs Inflammatory Bowel DiseaseДокумент2 страницыMcqs Inflammatory Bowel Diseaseiwennie100% (1)
- Guide To Medical Standards of Fitness To DriveДокумент53 страницыGuide To Medical Standards of Fitness To DriveiwennieОценок пока нет
- How To Read A CTGДокумент11 страницHow To Read A CTGiwennieОценок пока нет
- List of SpecialistsДокумент2 страницыList of SpecialistsiwennieОценок пока нет
- Xraysinent 170104125612Документ30 страницXraysinent 170104125612iwennieОценок пока нет
- The Menstrual CycleДокумент6 страницThe Menstrual CycleiwennieОценок пока нет
- المعدلات الطبيعية لمعظم الاختبارت بالمختبرДокумент4 страницыالمعدلات الطبيعية لمعظم الاختبارت بالمختبرMohamedErrmaliОценок пока нет
- Common Complications of PregnancyДокумент34 страницыCommon Complications of PregnancyiwennieОценок пока нет
- Lecture 1Документ75 страницLecture 1iwennieОценок пока нет
- BR J Hosp Med The Babinski SignДокумент8 страницBR J Hosp Med The Babinski SigniwennieОценок пока нет
- Weight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Документ1 страницаWeight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Malisa LukmanОценок пока нет
- Dimitris Loukopoulos PDFДокумент46 страницDimitris Loukopoulos PDFiwennieОценок пока нет
- IntroductionДокумент33 страницыIntroductioniwennieОценок пока нет
- Sterilization and DisinfectionДокумент3 страницыSterilization and DisinfectionAthul GurudasОценок пока нет
- Osteomalacia and RicketsДокумент4 страницыOsteomalacia and RicketsiwennieОценок пока нет
- Complication of TBДокумент15 страницComplication of TBTintin PoncianoОценок пока нет
- 3 Minute Exam of ChildrenДокумент2 страницы3 Minute Exam of ChildreniwennieОценок пока нет
- Pediatric Heart Failure 2015Документ7 страницPediatric Heart Failure 2015iwennieОценок пока нет
- Fluid, Electrolyte, and Acid-Base Balance IntroductionДокумент2 страницыFluid, Electrolyte, and Acid-Base Balance IntroductioniwennieОценок пока нет
- Blood DyscrasiaДокумент136 страницBlood DyscrasiaiwennieОценок пока нет
- Substance Use and Abuse Among AdolescentsДокумент9 страницSubstance Use and Abuse Among AdolescentsiwennieОценок пока нет
- Adolescent and YouthДокумент2 страницыAdolescent and YouthiwennieОценок пока нет
- Complication of TBДокумент15 страницComplication of TBTintin PoncianoОценок пока нет
- Pathology: Dr. Muriithi: 2 Year: 1 SemesterДокумент2 страницыPathology: Dr. Muriithi: 2 Year: 1 SemesteriwennieОценок пока нет
- Parasympathetic Vs Sympathetic Nervous System - Difference and ComparisonДокумент4 страницыParasympathetic Vs Sympathetic Nervous System - Difference and ComparisoniwennieОценок пока нет
- Aneamis and HaematologyДокумент129 страницAneamis and HaematologyiwennieОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Research ProposalДокумент45 страницResearch ProposalBoruuf If GammachuuОценок пока нет
- ENGLISH VERSION - Lactation Teaching ToolsДокумент15 страницENGLISH VERSION - Lactation Teaching ToolsXiomara Salort100% (1)
- Pregnancy W Std's ArticleДокумент4 страницыPregnancy W Std's ArticleCharina AubreyОценок пока нет
- Summative Test 1 in Science 5 2nd QuarterДокумент4 страницыSummative Test 1 in Science 5 2nd Quarterfrancisann.constanteОценок пока нет
- Reproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Документ50 страницReproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Vesna AntovskaОценок пока нет
- Hellp Syndrome ArticleДокумент8 страницHellp Syndrome ArticleDIANNE FAYE LARAGANОценок пока нет
- Breast FeedingДокумент33 страницыBreast Feedingjulie kisku100% (1)
- Rcog PretermДокумент13 страницRcog Pretermsintiadamayanti100% (1)
- Family Planning MethodsДокумент7 страницFamily Planning MethodsAngelika PadawanОценок пока нет
- Dr Kanadi Sumapraja discusses recurrent pregnancy loss managementДокумент63 страницыDr Kanadi Sumapraja discusses recurrent pregnancy loss managementNetty HerawatiОценок пока нет
- Rhinessa Women's Q EnglishДокумент8 страницRhinessa Women's Q EnglishDavis ShirleyОценок пока нет
- Topic 9 ObsДокумент7 страницTopic 9 ObsHannan SyedОценок пока нет
- Fetal Heart Monitoring AWHONN 15Документ4 страницыFetal Heart Monitoring AWHONN 15Álvaro M. Luna CisnerosОценок пока нет
- ObstetricsДокумент7 страницObstetricsArleneDelosSantos100% (1)
- Preterm Labor ManagementДокумент50 страницPreterm Labor ManagementDr-Firas Nayf Al-ThawabiaОценок пока нет
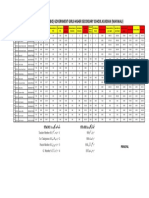
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Документ1 страницаMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadОценок пока нет
- Abortion PP TДокумент42 страницыAbortion PP TDivya ToppoОценок пока нет
- IVFДокумент168 страницIVFAbhishek Vijayakumar100% (3)
- Managing Malpositions of the Fetal HeadДокумент8 страницManaging Malpositions of the Fetal HeaduouoОценок пока нет
- Lesson Plan: Female Hormonal CyclesДокумент9 страницLesson Plan: Female Hormonal CyclesGunaОценок пока нет
- BBLRДокумент37 страницBBLRHernina OktavianiОценок пока нет
- Breast Cancer and Pregnancy: How To Proceed?Документ3 страницыBreast Cancer and Pregnancy: How To Proceed?IJAR JOURNALОценок пока нет
- An Integrated Approach To Fetal Growth RestrictionДокумент11 страницAn Integrated Approach To Fetal Growth RestrictionalexandraОценок пока нет
- In Vitro Fertilization (Ivf)Документ2 страницыIn Vitro Fertilization (Ivf)allfonsoОценок пока нет
- Family Planning (Teaching Plan) Ana AlcasabasДокумент6 страницFamily Planning (Teaching Plan) Ana Alcasabasiammerbinpransisko75% (4)
- Screening of Breast CancerДокумент19 страницScreening of Breast CancerIncredible DivineОценок пока нет
- AbortionДокумент92 страницыAbortionniraj_sdОценок пока нет
- Birth Preparedness HandbookДокумент338 страницBirth Preparedness HandbookPrabir Kumar Chatterjee100% (2)
- Lactational Amenorrhea Method (LAM)Документ10 страницLactational Amenorrhea Method (LAM)Jovie May Adversalo100% (1)
- Maternal and Child Health NursingДокумент25 страницMaternal and Child Health Nursingmarie100% (46)