Вам также может понравиться
- Trichotillomania FIXДокумент13 страницTrichotillomania FIXVeronica Yosita AnandaОценок пока нет
- Trichotillomania: Supervisor: Dokter Iwan Sys, SP - KJДокумент13 страницTrichotillomania: Supervisor: Dokter Iwan Sys, SP - KJVeronica Yosita AnandaОценок пока нет
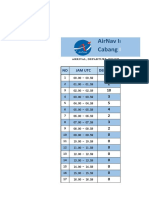
- Grafik Laporan Operasi18 - OKTOBERДокумент56 страницGrafik Laporan Operasi18 - OKTOBERVeronica Yosita AnandaОценок пока нет
- Penyuluhan CemasДокумент7 страницPenyuluhan CemasVeronica Yosita AnandaОценок пока нет
- Delirium Tremens TugasДокумент14 страницDelirium Tremens TugasVeronica Yosita AnandaОценок пока нет
- Relationship of Smartphone Use Severity With Sleep Quality, Depression, and Anxiety in University StudentsДокумент8 страницRelationship of Smartphone Use Severity With Sleep Quality, Depression, and Anxiety in University StudentsVeronica Yosita AnandaОценок пока нет
- Research Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseДокумент13 страницResearch Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseVeronica Yosita AnandaОценок пока нет
- Psoriasis: Journal ReadingДокумент13 страницPsoriasis: Journal ReadingVeronica Yosita AnandaОценок пока нет
- Diare Akut: Adhesi Invasi Sitotoksin EnterotoksinДокумент4 страницыDiare Akut: Adhesi Invasi Sitotoksin EnterotoksinVeronica Yosita AnandaОценок пока нет
- Dry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGДокумент3 страницыDry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGVeronica Yosita AnandaОценок пока нет
- Frequency Table: PasarДокумент6 страницFrequency Table: PasarVeronica Yosita AnandaОценок пока нет
- Jadwal Jaga Stase Bedah Clekship FK UmmДокумент1 страницаJadwal Jaga Stase Bedah Clekship FK UmmVeronica Yosita AnandaОценок пока нет
- List Obat Baksos (100 Pasien)Документ3 страницыList Obat Baksos (100 Pasien)Veronica Yosita AnandaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Pathophysiology Dyslipidemia PDFДокумент9 страницPathophysiology Dyslipidemia PDFtiffa07110% (1)
- CA 2 - CHN Review 50 Items PretestДокумент10 страницCA 2 - CHN Review 50 Items PretestAlibasher Macalnas100% (1)
- Food Related DiseasesДокумент19 страницFood Related DiseasesCabdullahi maxamed xussenОценок пока нет
- Fitness Progress Chart For Men (Metric)Документ4 страницыFitness Progress Chart For Men (Metric)Marius MitricăОценок пока нет
- Aun Herbal CatalogДокумент29 страницAun Herbal Catalogaunherbalremedies2009Оценок пока нет
- Surchod MiphamДокумент13 страницSurchod MiphamShenphen Ozer100% (1)
- Dr. Max Gerson Inducted Into Orthomolecular Medicine Hall of Fame - 2005Документ2 страницыDr. Max Gerson Inducted Into Orthomolecular Medicine Hall of Fame - 2005TUartistОценок пока нет
- NCP - BronchopneumoniaДокумент11 страницNCP - BronchopneumoniaMaria Ivy Mendoza100% (1)
- What Causes Dizziness With NauseaДокумент10 страницWhat Causes Dizziness With NauseaDori BarreirosОценок пока нет
- Kolelitiasis in EnglishДокумент18 страницKolelitiasis in EnglishReza AkbarОценок пока нет
- 06 - RLE - Infection Prevention and ControlДокумент1 страница06 - RLE - Infection Prevention and ControlERICKA CASANDRA MASLOG ABASОценок пока нет
- Journal GastroenterologyДокумент14 страницJournal GastroenterologySusilo PrihrantoОценок пока нет
- 300 Items NLE ReviewerДокумент47 страниц300 Items NLE Reviewercesspintas CuaresmaОценок пока нет
- Special Procudure (UGIS) : Body Habitus HyposthenicДокумент12 страницSpecial Procudure (UGIS) : Body Habitus HyposthenicJoeriz Bartolome100% (1)
- ShejayLomongo BSN2Документ15 страницShejayLomongo BSN2Shejay LomongoОценок пока нет
- Acute Gastroenteritis (AGE) : A Case Study ONДокумент9 страницAcute Gastroenteritis (AGE) : A Case Study ONMay Ann Magdaraog ArdamilОценок пока нет
- Aspirin OverdoseДокумент3 страницыAspirin OverdoseSaputra BismaОценок пока нет
- Enteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)Документ3 страницыEnteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)fildzah amalyaОценок пока нет
- Notes From Beynon LectureДокумент6 страницNotes From Beynon LecturearianОценок пока нет
- McqsДокумент15 страницMcqsNazaqat FarooqОценок пока нет
- 01 Disorders and Diseases of The Human Reproductive SystemДокумент7 страниц01 Disorders and Diseases of The Human Reproductive SystemAlwaysSaugstОценок пока нет
- Surveillance System in The PhilippinesДокумент38 страницSurveillance System in The PhilippinesFred C. MirandaОценок пока нет
- Fluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Документ87 страницFluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Siyum MathewosОценок пока нет
- Drug Study - LosartanДокумент2 страницыDrug Study - LosartanCath Bril50% (2)
- Benchmark Disability As Defined Under Section 2 (R) of The RPWD Act, 2016 and Has LimitationДокумент1 страницаBenchmark Disability As Defined Under Section 2 (R) of The RPWD Act, 2016 and Has LimitationVidhiLegal BlogОценок пока нет
- Atlas of Geriatric Dermatology 2013 - PDF - DR - Carson - VRGДокумент334 страницыAtlas of Geriatric Dermatology 2013 - PDF - DR - Carson - VRGANÔNIMOОценок пока нет
- 54kKNm PDFДокумент18 страниц54kKNm PDFFikriwbОценок пока нет
- Surgery QuestionsДокумент312 страницSurgery Questionsmonaliza7100% (9)
- Test Pitanja Iz Respiratornog Sistema Sa PrevodomДокумент10 страницTest Pitanja Iz Respiratornog Sistema Sa PrevodomzerohajdukОценок пока нет
- Natural RemediesДокумент29 страницNatural RemediesAmit Kumar Sen100% (2)