Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Test Dos InglesДокумент4 страницыTest Dos Inglesgbøniillaa75% (4)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Chicken Wing DissectionДокумент13 страницChicken Wing DissectionJaga_Sahsiny_1Оценок пока нет
- The ScarecrowДокумент5 страницThe ScarecrowJuvent0% (1)
- CohotДокумент14 страницCohotMadyline VictoryaОценок пока нет
- Gizi SeimbangДокумент54 страницыGizi SeimbangMarliana PohanОценок пока нет
- AP MR GlossaryДокумент5 страницAP MR GlossaryReynaldi HadiwijayaОценок пока нет
- 455657Документ2 страницы455657Madyline VictoryaОценок пока нет
- KKR - 8 Mei 2014Документ2 страницыKKR - 8 Mei 2014Madyline VictoryaОценок пока нет
- Age Ageing-2013 - I1-I57Документ57 страницAge Ageing-2013 - I1-I57Madyline VictoryaОценок пока нет
- Jadwal Piket Perawat Rawat IanapДокумент18 страницJadwal Piket Perawat Rawat IanapMadyline Victorya100% (1)
- Adosex 1Документ52 страницыAdosex 1Madyline VictoryaОценок пока нет
- SpiritualityДокумент82 страницыSpiritualityMadyline VictoryaОценок пока нет
- The Secrets of Long LifeДокумент10 страницThe Secrets of Long LifeMadyline VictoryaОценок пока нет
- Paincontrol PDFДокумент52 страницыPaincontrol PDFMadyline VictoryaОценок пока нет
- Standards of Good Practice For Spinal Interventional ProceduresДокумент20 страницStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaОценок пока нет
- Sofa Score PDFДокумент4 страницыSofa Score PDFMadyline VictoryaОценок пока нет
- 2006 8215Документ86 страниц2006 8215Madyline VictoryaОценок пока нет
- Referat RadiologiДокумент6 страницReferat RadiologiMadyline VictoryaОценок пока нет
- EmpyemaДокумент27 страницEmpyemaMadyline VictoryaОценок пока нет
- Journal ReadingДокумент23 страницыJournal ReadingMadyline VictoryaОценок пока нет
- Anestesi and FESSДокумент6 страницAnestesi and FESSMadyline VictoryaОценок пока нет
- NelsonДокумент1 страницаNelsonMadyline VictoryaОценок пока нет
- Basic Life SupportДокумент12 страницBasic Life SupportMadyline VictoryaОценок пока нет
- The Secrets of Long LifeДокумент10 страницThe Secrets of Long LifeMadyline VictoryaОценок пока нет
- Ectopic PregnancyДокумент16 страницEctopic PregnancyMadyline VictoryaОценок пока нет
- Socialism CapitalismДокумент268 страницSocialism CapitalismRobert PattonОценок пока нет
- Standards of Good Practice For Spinal Interventional ProceduresДокумент20 страницStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaОценок пока нет
- Cardiology Research EvaluationДокумент6 страницCardiology Research EvaluationMadyline VictoryaОценок пока нет
- Hasil Kontrol LisaДокумент2 страницыHasil Kontrol LisaMadyline VictoryaОценок пока нет
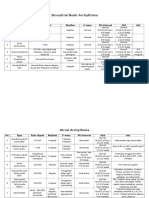
- Sinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetДокумент3 страницыSinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetMadyline VictoryaОценок пока нет
- Pain Assess Breakthrough Pain HagenДокумент8 страницPain Assess Breakthrough Pain HagenMadyline VictoryaОценок пока нет
- Pub Prof EpiduralAnalgesia2010Документ14 страницPub Prof EpiduralAnalgesia2010Madyline VictoryaОценок пока нет
- ImpressionДокумент7 страницImpressionAnnisa Nur AmalaОценок пока нет
- CrocodilesДокумент3 страницыCrocodilesPeculiarMemoriesОценок пока нет
- Jack's Head (Siggy Shade)Документ101 страницаJack's Head (Siggy Shade)parikhaastha1804Оценок пока нет
- Vis The Ruffianly Bitch and A Pair of Grim Shaggy Sheep-Dogs, Who SharedДокумент10 страницVis The Ruffianly Bitch and A Pair of Grim Shaggy Sheep-Dogs, Who SharedChris BartlettОценок пока нет
- Catclass NotesДокумент3 страницыCatclass NotesIssac CaldwellОценок пока нет
- Cat and Mouse 2Документ2 страницыCat and Mouse 2Da MiánОценок пока нет
- PL Pritomny Priebehovy CasДокумент6 страницPL Pritomny Priebehovy CasSimivis SimОценок пока нет
- Diagnosis of Viral Infections in Animal TissuesДокумент3 страницыDiagnosis of Viral Infections in Animal TissuesRandy Butternubs100% (2)
- Lethal Dose 50Документ18 страницLethal Dose 50h3cn1r3Оценок пока нет
- a hero of our time (当代英雄)Документ165 страницa hero of our time (当代英雄)JingОценок пока нет
- Chaparrí: Ubicación: Región Lambayeque. Provincia de Chiclayo, Distrito de Chongoyape, Caserío TierrasДокумент3 страницыChaparrí: Ubicación: Región Lambayeque. Provincia de Chiclayo, Distrito de Chongoyape, Caserío TierrasAlexs TomapascaОценок пока нет
- Serotonergic Neurotransmission in Mediating Social Behavior in Octopus PDFДокумент31 страницаSerotonergic Neurotransmission in Mediating Social Behavior in Octopus PDFbugmenomoreОценок пока нет
- GG BA Honours Semester 2 Ode On The Death of A Favourite Cat Lecture 1Документ15 страницGG BA Honours Semester 2 Ode On The Death of A Favourite Cat Lecture 1archana anilОценок пока нет
- Horse Welfare CompendiumДокумент76 страницHorse Welfare CompendiumbodnarencoОценок пока нет
- Class 3 EVS Question Bank 1Документ8 страницClass 3 EVS Question Bank 1ᴅᴇᴇᴘ ᴘʀᴀᴋᴀsʜ ᴍᴏᴅɪ xɪ-ᴅОценок пока нет
- Activity Book 1º - EstudianteДокумент89 страницActivity Book 1º - EstudianteJULIO CESARОценок пока нет
- Properties of LanguageДокумент2 страницыProperties of LanguageNurul IzzatiОценок пока нет
- Aulia Rahmatun Nufus Raihanun Nisa Dinur Sri RizkiДокумент18 страницAulia Rahmatun Nufus Raihanun Nisa Dinur Sri RizkiFauzan JakfarОценок пока нет
- Chapter-2 Profile of Karbi Anglong DistrictДокумент37 страницChapter-2 Profile of Karbi Anglong DistrictDiganta Kumar GogoiОценок пока нет
- Tibetan Personality TestДокумент19 страницTibetan Personality TestIan VarelaОценок пока нет
- Tuberculosis: What Is It and How Do We Keep Healthy?: A Presentation For Pacific Island Schools and CommunitiesДокумент17 страницTuberculosis: What Is It and How Do We Keep Healthy?: A Presentation For Pacific Island Schools and CommunitiesKailash NagarОценок пока нет
- Anatomy and Physiology of The EyesДокумент20 страницAnatomy and Physiology of The EyesLaidy Aizahlyn Indoc Angod100% (2)
- Microsoft Word - The BloodДокумент16 страницMicrosoft Word - The BloodMelanie Fleckner0% (3)
- Exam (1) On Unit (1) :: Connect Plus 4 - 1st TermДокумент12 страницExam (1) On Unit (1) :: Connect Plus 4 - 1st TermHassan k1455 rashidОценок пока нет
- National Geographic Little Kids - 03 2019 - 04 2019Документ35 страницNational Geographic Little Kids - 03 2019 - 04 2019florenciaОценок пока нет
- Cell As The Basic Unit of LifeДокумент48 страницCell As The Basic Unit of Lifeharshana rajagopalОценок пока нет
- WonderlandДокумент2 страницыWonderlandJohn WilliamsОценок пока нет