Вам также может понравиться
- Cielito Lindo Violin IДокумент1 страницаCielito Lindo Violin IArturo Manuel Garza Ramos MonroyОценок пока нет
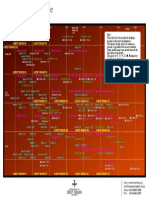
- Trumpet Mouthpieces Comparison Chart PDFДокумент1 страницаTrumpet Mouthpieces Comparison Chart PDFArturo GarzaОценок пока нет
- French Studies Volume Xxxiv Issue 4 1980 (Doi 10.1093 - Fs - Xxxiv.4.422) Greene, Robert W. - Fluency, Muteness and Commitment in Camus's La PesteДокумент12 страницFrench Studies Volume Xxxiv Issue 4 1980 (Doi 10.1093 - Fs - Xxxiv.4.422) Greene, Robert W. - Fluency, Muteness and Commitment in Camus's La PesteArturo Manuel Garza Ramos MonroyОценок пока нет
- Assessing Narrative Comprehension in Young ChildrenДокумент41 страницаAssessing Narrative Comprehension in Young ChildrenArturo Manuel Garza Ramos Monroy100% (1)
- J.S. Mackley - The Legend of ST Brendan - A Comparative Study of The Latin and Anglo-Norman Versions (The Northern World) - Brill Academic Publishers (2008)Документ367 страницJ.S. Mackley - The Legend of ST Brendan - A Comparative Study of The Latin and Anglo-Norman Versions (The Northern World) - Brill Academic Publishers (2008)Arturo Manuel Garza Ramos Monroy67% (3)
- (the Northern World 24) Glyn S. Burgess, Clara Strijbosch - The Brendan Legend_ Texts and Versions (the Northern World_ North Europe and the Baltic C.400-1700 Ad_ Peoples, Economies and Cultures)-BrilДокумент405 страниц(the Northern World 24) Glyn S. Burgess, Clara Strijbosch - The Brendan Legend_ Texts and Versions (the Northern World_ North Europe and the Baltic C.400-1700 Ad_ Peoples, Economies and Cultures)-BrilArturo Manuel Garza Ramos Monroy100% (2)
- 59784-Artikkelin Teksti-63334-1-10-20161202Документ9 страниц59784-Artikkelin Teksti-63334-1-10-20161202Arturo Manuel Garza Ramos MonroyОценок пока нет
- Scott G. Paris, Linda R. Ayres - Becoming Reflective Students and Teachers With Portfolios and Authentic Assessment (Psychology in the Classroom _ a Series on Applied Educational Psy) (1994, American Psychological AДокумент181 страницаScott G. Paris, Linda R. Ayres - Becoming Reflective Students and Teachers With Portfolios and Authentic Assessment (Psychology in the Classroom _ a Series on Applied Educational Psy) (1994, American Psychological AArturo Manuel Garza Ramos Monroy100% (1)
- Dialnet TrainingFunctionalTranslators 4925497 PDFДокумент20 страницDialnet TrainingFunctionalTranslators 4925497 PDFArturo Manuel Garza Ramos MonroyОценок пока нет
- Scott G. Paris, Linda R. Ayres - Becoming Reflective Students and Teachers With Portfolios and Authentic Assessment (Psychology in the Classroom _ a Series on Applied Educational Psy) (1994, American Psychological AДокумент181 страницаScott G. Paris, Linda R. Ayres - Becoming Reflective Students and Teachers With Portfolios and Authentic Assessment (Psychology in the Classroom _ a Series on Applied Educational Psy) (1994, American Psychological AArturo Manuel Garza Ramos Monroy100% (1)
- W215R12 Trumpets EuДокумент28 страницW215R12 Trumpets EuArturo Manuel Garza Ramos Monroy100% (3)
- Vizzutti 1Документ128 страницVizzutti 1Arturo Manuel Garza Ramos MonroyОценок пока нет
- Yamaha Mouthpiece Guide PDFДокумент36 страницYamaha Mouthpiece Guide PDFgirard_boweОценок пока нет
- A Phenomenological Approach To Jazz Improvisation PDFДокумент46 страницA Phenomenological Approach To Jazz Improvisation PDFArturo Manuel Garza Ramos MonroyОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Fastners and Allied Products Pvt. Ltd.Документ79 страницFastners and Allied Products Pvt. Ltd.KeerthiОценок пока нет
- Business ResearchsampleДокумент38 страницBusiness Researchsamplebasma ezzatОценок пока нет
- Workforce Planning and Staffing MetricsДокумент25 страницWorkforce Planning and Staffing MetricsKashika100% (1)
- Recruitment: By: Soundouss Belekbir Zineb El Akkati Manal Nasihi Mehdi LyazidiДокумент29 страницRecruitment: By: Soundouss Belekbir Zineb El Akkati Manal Nasihi Mehdi LyazidiNafia AbdrrahmanОценок пока нет
- Manpower Planning Is A Very Important Component of HR ManagementДокумент7 страницManpower Planning Is A Very Important Component of HR Managementwasim2011Оценок пока нет
- Chapter 3 Attitudes and Job Satisfaction Multiple ChoiceДокумент19 страницChapter 3 Attitudes and Job Satisfaction Multiple Choicehesham hassanОценок пока нет
- Shouldice Hospital - A Case StudyДокумент44 страницыShouldice Hospital - A Case StudyPimkhwan_Bunji_2272100% (1)
- Employee BenefitsДокумент59 страницEmployee BenefitsumarmasoodОценок пока нет
- A Study On Overview of Employee Attrition Rate in India 150759937Документ5 страницA Study On Overview of Employee Attrition Rate in India 150759937Pramit NarayanОценок пока нет
- Learn key job attitudes like satisfaction, involvement and commitmentДокумент40 страницLearn key job attitudes like satisfaction, involvement and commitmentZulkifli FadhilahОценок пока нет
- Flexible Work SchedulesДокумент11 страницFlexible Work SchedulesМария НиколенкоОценок пока нет
- Recommendation ReportДокумент16 страницRecommendation ReportAmanda MejiaОценок пока нет
- Peer Graded AssignmentДокумент2 страницыPeer Graded AssignmentBobby RoyОценок пока нет
- Summer Project ReportДокумент198 страницSummer Project Report1469 Tirth VekariyaОценок пока нет
- Toxic Work Environment EbookДокумент21 страницаToxic Work Environment EbookNicole L. Turner100% (1)
- Industrial Democracy Significance: Principles of Personnel Management LessonДокумент7 страницIndustrial Democracy Significance: Principles of Personnel Management LessonBT21EC018 Harsh SharmaОценок пока нет
- 10 DEI Metrics Your Organization Should Track - AIHRДокумент17 страниц10 DEI Metrics Your Organization Should Track - AIHRluesbagoОценок пока нет
- The Assesiment of Staff Turnover atДокумент69 страницThe Assesiment of Staff Turnover atMitiku ShewaОценок пока нет
- Delegation-Making The Most of The Gift of Time: Gail ThomasДокумент3 страницыDelegation-Making The Most of The Gift of Time: Gail ThomasBusiness Expert PressОценок пока нет
- Occupational Stress in The Hospitality IndustryДокумент26 страницOccupational Stress in The Hospitality IndustrySumitha GОценок пока нет
- Employment RelationsДокумент22 страницыEmployment Relationsalia awatifОценок пока нет
- BrownДокумент13 страницBrownapi-255084253Оценок пока нет
- Performance Management at Vitality HealthДокумент7 страницPerformance Management at Vitality HealthRachit Pradhan33% (3)
- Chapter 2 Quiz and Answer Keys Training and DevelopmentДокумент25 страницChapter 2 Quiz and Answer Keys Training and DevelopmentEwura Esi Eyram Aboagyewaa100% (1)
- HRM All Case DoneДокумент33 страницыHRM All Case Donearif98771% (7)
- Exit Interview in Relation To Employer Branding. - REPORTДокумент81 страницаExit Interview in Relation To Employer Branding. - REPORTPreethu Gowda100% (5)
- Employee Retention and Well Being Issue AДокумент9 страницEmployee Retention and Well Being Issue AAnshita100% (1)
- Techniques of HRMДокумент14 страницTechniques of HRMBelur Baxi100% (1)
- Gender Diversity in the WorkplaceДокумент18 страницGender Diversity in the WorkplaceJamie BagundolОценок пока нет
- Attrition in Indian BPO IndustryДокумент19 страницAttrition in Indian BPO IndustrySushil BaralОценок пока нет