Вам также может понравиться
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderОт EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderОценок пока нет
- Rotational Flap Closure of 1st and 5nth Met HeadДокумент8 страницRotational Flap Closure of 1st and 5nth Met HeadleahbayОценок пока нет
- 2002, Vol.33, Issues 1, Treatment of Complex FracturesДокумент280 страниц2002, Vol.33, Issues 1, Treatment of Complex FracturesSitthikorn StrikerrОценок пока нет
- Ten Questions On Kienbock's DiseaseДокумент6 страницTen Questions On Kienbock's DiseaseProfesseur Christian DumontierОценок пока нет
- Cavovarus Foot JOT 2018Документ5 страницCavovarus Foot JOT 2018Noel Yongshen LeeОценок пока нет
- Pilon Fractures Preventing ComplicationsДокумент12 страницPilon Fractures Preventing ComplicationsjojoОценок пока нет
- Surgical Approach To Hand and Wrist PDFДокумент76 страницSurgical Approach To Hand and Wrist PDFForminte MarianОценок пока нет
- Clinicas de Endocrino. Pie Diabetico - Dic 2013Документ15 страницClinicas de Endocrino. Pie Diabetico - Dic 2013Betzabeth RodriguezОценок пока нет
- Clemens Attinger 10 Angiosomes and Wound Care in The Diabetic FootДокумент26 страницClemens Attinger 10 Angiosomes and Wound Care in The Diabetic FootDorin DvornicОценок пока нет
- The Journal of Bangladesh Orthopaedic Society (JBOS)Документ118 страницThe Journal of Bangladesh Orthopaedic Society (JBOS)Roman Popescu100% (1)
- Outpatientassessmentand Managementofthediabeticfoot: John A. DipretaДокумент21 страницаOutpatientassessmentand Managementofthediabeticfoot: John A. DipretaAnonymous kdBDppigEОценок пока нет
- External Fixation Principles and Applications.5Документ8 страницExternal Fixation Principles and Applications.5Leonardo Rocha100% (1)
- Diabetic Foot InfectionsДокумент52 страницыDiabetic Foot Infectionsshivakumar52Оценок пока нет
- Cavus Foot: Monica Paschoal Nogueira,, Fernando Farcetta,, Alexandre ZucconДокумент12 страницCavus Foot: Monica Paschoal Nogueira,, Fernando Farcetta,, Alexandre ZucconCesar AlvaradoОценок пока нет
- Juvenile Hallux Valgus PDFДокумент14 страницJuvenile Hallux Valgus PDFŞtefaniuc IulianОценок пока нет
- Foot and Ankle Clinics Volume A Refined Classification SystemДокумент17 страницFoot and Ankle Clinics Volume A Refined Classification SystemRicardo CastilloОценок пока нет
- AAOS - Clubfoot - ADCДокумент17 страницAAOS - Clubfoot - ADCMulya ImansyahОценок пока нет
- Review - Presby Residency ManualДокумент400 страницReview - Presby Residency ManualSneha SutharОценок пока нет
- Can Nanotechnology Help To Repair The BodyДокумент27 страницCan Nanotechnology Help To Repair The BodyPaulo Henrique MuzekaОценок пока нет
- Diagnosis and Treatment of Acute Essex-Lopresti inДокумент11 страницDiagnosis and Treatment of Acute Essex-Lopresti inMỸ NGUYỄN CÔNGОценок пока нет
- Shoulder Arthroplasty WIC - Dr. LSДокумент56 страницShoulder Arthroplasty WIC - Dr. LSDifitasari Cipta Perdana100% (1)
- OITE ReviewДокумент154 страницыOITE ReviewPanagiotis Poulios100% (2)
- DNB Questions Year Wise KNДокумент15 страницDNB Questions Year Wise KNphr3056Оценок пока нет
- Club Foot PDFДокумент54 страницыClub Foot PDFBelle Sakunrat SarikitОценок пока нет
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSДокумент20 страницDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeОценок пока нет
- All Papers Topic WiseДокумент55 страницAll Papers Topic WiseZ TariqОценок пока нет
- Charnley Ankle ArthrodesisДокумент12 страницCharnley Ankle Arthrodesisdr_s_ganeshОценок пока нет
- Curbside Consultation in Knee Arthroplasty 49 Clinical QuestionsДокумент230 страницCurbside Consultation in Knee Arthroplasty 49 Clinical QuestionsBane StarcevicОценок пока нет
- Osteotomias PediatriaДокумент13 страницOsteotomias PediatriaM Ram CrraОценок пока нет
- Kamars RadiologyДокумент135 страницKamars RadiologyNayantara Nair100% (1)
- OSTEOTOMIES AROUND THE HIP FinalДокумент51 страницаOSTEOTOMIES AROUND THE HIP FinalWasim R. IssaОценок пока нет
- Acute Distal Radioulnar Joint InstabilityДокумент13 страницAcute Distal Radioulnar Joint Instabilityyerson fernando tarazona tolozaОценок пока нет
- Limb Reconstruction SystemДокумент83 страницыLimb Reconstruction SystemGermán0% (1)
- PDFДокумент328 страницPDFBreak DerulsОценок пока нет
- Acute Carpal Tunnel Syndrome: A Review of Current LiteratureДокумент9 страницAcute Carpal Tunnel Syndrome: A Review of Current LiteratureUlos BenardОценок пока нет
- Modified French OsteotomyДокумент5 страницModified French OsteotomyKaustubh KeskarОценок пока нет
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsДокумент7 страницTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersОценок пока нет
- DRUJinstabilityreview - PDF 034407Документ15 страницDRUJinstabilityreview - PDF 034407Oscar Cayetano Herrera RodríguezОценок пока нет
- Syllabus Ms OrthoДокумент8 страницSyllabus Ms OrthoMuthu KumarОценок пока нет
- Resource Unit Wound Care EnglishДокумент5 страницResource Unit Wound Care EnglishPeterOrlinoОценок пока нет
- James P. Stannard Et La - Knee Surgery Tricks of The TradeДокумент739 страницJames P. Stannard Et La - Knee Surgery Tricks of The TradeFernanda NoraОценок пока нет
- A Systematic Approach To The Hip-Spine Relationship and Its Applications To Total Hip Arthroplasty - Eftekhary Et Al. 2019Документ9 страницA Systematic Approach To The Hip-Spine Relationship and Its Applications To Total Hip Arthroplasty - Eftekhary Et Al. 2019Mohammad KaramОценок пока нет
- Management Tibial Plateau FractureДокумент45 страницManagement Tibial Plateau FracturePurushothama Rao NalamatiОценок пока нет
- AdultHip Abstracts PDFДокумент106 страницAdultHip Abstracts PDFJafild Fild riverОценок пока нет
- 22 Gait DisordersДокумент13 страниц22 Gait DisordersAbhilekh SrivastavaОценок пока нет
- AAOS2007 Pediatric PDFДокумент58 страницAAOS2007 Pediatric PDFHéctor Pando SánchezОценок пока нет
- Hardinge ModifiedДокумент5 страницHardinge ModifiedscribdfoaktОценок пока нет
- PMR Role in Congenital Limb Deficient 2Документ42 страницыPMR Role in Congenital Limb Deficient 2virginiaОценок пока нет
- Hip OsteotmyДокумент4 страницыHip OsteotmyAhmed KeshkОценок пока нет
- Long Case OrthopaedicДокумент24 страницыLong Case OrthopaedicSyimah UmarОценок пока нет
- Arthroscopic Ankle ArthrodesisДокумент37 страницArthroscopic Ankle ArthrodesisJan VelosoОценок пока нет
- Above-Knee Fitting and Alignment Tehniques PDFДокумент18 страницAbove-Knee Fitting and Alignment Tehniques PDFsunsrayОценок пока нет
- CHAPTER 14 - Treatment of Bone Def - 2008 - Surgical Techniques of The ShoulderДокумент11 страницCHAPTER 14 - Treatment of Bone Def - 2008 - Surgical Techniques of The ShoulderJaime Vázquez ZárateОценок пока нет
- Journal ReadingДокумент7 страницJournal ReadingTommy HardiantoОценок пока нет
- Pelvic Osteotomies in The Child and Young Adult Hip: Indications and Surgical TechniqueДокумент8 страницPelvic Osteotomies in The Child and Young Adult Hip: Indications and Surgical TechniqueLeonardo Guerrero CardozoОценок пока нет
- AAOS Mini Open Rotator Cuff RepairДокумент10 страницAAOS Mini Open Rotator Cuff RepairHannah CoОценок пока нет
- Gpe - 017.1 - Orthopaedic ExaminationДокумент3 страницыGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumОценок пока нет
- The Osteoporotic Syndrome: Detection, Prevention, and TreatmentОт EverandThe Osteoporotic Syndrome: Detection, Prevention, and TreatmentОценок пока нет
- Table of ContentsДокумент2 страницыTable of ContentsAngelica Mercado SirotОценок пока нет
- Saint Louis University: Application FormДокумент4 страницыSaint Louis University: Application FormAngelica Mercado SirotОценок пока нет
- Ja ChimoДокумент28 страницJa ChimotwinkletwinkleОценок пока нет
- Communication - Public SpeakingДокумент19 страницCommunication - Public SpeakingAngelica Mercado SirotОценок пока нет
- Eng Elec ArticleДокумент1 страницаEng Elec ArticleAngelica Mercado SirotОценок пока нет
- Lesson Plan On CPRДокумент9 страницLesson Plan On CPRAngelica Mercado SirotОценок пока нет
- Access Letter Requesting Permission To Conduct Research 4Документ7 страницAccess Letter Requesting Permission To Conduct Research 4Angelica Mercado SirotОценок пока нет
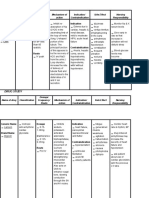
- Drug Study FinalДокумент21 страницаDrug Study FinalAngelica Mercado SirotОценок пока нет
- Respiratory FailureДокумент7 страницRespiratory FailureAngelica Mercado SirotОценок пока нет
- Angel's ResearchДокумент1 страницаAngel's ResearchAngelica Mercado SirotОценок пока нет
- Questionnaire With FeedbackДокумент4 страницыQuestionnaire With FeedbackAngelica Mercado SirotОценок пока нет
- Olivarez College Dr. Arcadio Santos Avenue, Sucat Road, Parañaque City College of NursingДокумент1 страницаOlivarez College Dr. Arcadio Santos Avenue, Sucat Road, Parañaque City College of NursingAngelica Mercado SirotОценок пока нет
- Course in The WardДокумент5 страницCourse in The WardAngelica Mercado SirotОценок пока нет
- What A Wonderful World Janus-Suit Choir - Floral: T-Shirt Sa LoobДокумент2 страницыWhat A Wonderful World Janus-Suit Choir - Floral: T-Shirt Sa LoobAngelica Mercado SirotОценок пока нет
- 2011 Dotted CalendarsДокумент12 страниц2011 Dotted CalendarsPenny WaddinghamОценок пока нет
- Narrative Report TPMCДокумент1 страницаNarrative Report TPMCAngelica Mercado Sirot100% (1)
- Ref L IctionДокумент1 страницаRef L IctionAngelica Mercado SirotОценок пока нет
- IntroductionДокумент1 страницаIntroductionAngelica Mercado SirotОценок пока нет
- Nolimetangerescript1 FinalДокумент53 страницыNolimetangerescript1 FinalAngelica Mercado SirotОценок пока нет
- Nolimetangerescript1 FinalДокумент53 страницыNolimetangerescript1 FinalAngelica Mercado SirotОценок пока нет
- Congestive Heart Failure (Pathophysiology)Документ1 страницаCongestive Heart Failure (Pathophysiology)Angelica Mercado SirotОценок пока нет
- NCP AfДокумент3 страницыNCP AfAngelica Mercado SirotОценок пока нет
- DRUG STUDY (Ma'am D)Документ3 страницыDRUG STUDY (Ma'am D)Angelica Mercado SirotОценок пока нет
- NCPДокумент3 страницыNCPMichelle TamorОценок пока нет
- Anemia For ChronicДокумент28 страницAnemia For ChronicRetma Rosela NurkayantyОценок пока нет
- Scholastic Triumphs at Ateneo de ManilaДокумент2 страницыScholastic Triumphs at Ateneo de ManilaAngelica Mercado SirotОценок пока нет
- Name of DrugДокумент2 страницыName of DrugAngelica Mercado SirotОценок пока нет
- Checklist ToolДокумент3 страницыChecklist ToolAngelica Mercado SirotОценок пока нет
- Anemia For ChronicДокумент28 страницAnemia For ChronicRetma Rosela NurkayantyОценок пока нет
- Perineal HematomДокумент11 страницPerineal HematomLance TapelОценок пока нет
- OZ 02 The Marvelous Land of OzДокумент62 страницыOZ 02 The Marvelous Land of Ozbunnycat666Оценок пока нет
- Exceptional DevelopmentДокумент12 страницExceptional DevelopmentMa. IvoryVan SantillanОценок пока нет
- Dust Test Kit Sp3200 - d44Документ2 страницыDust Test Kit Sp3200 - d44Shenhua Kronen SohneОценок пока нет
- 1224 Threading Machine - Operator's Manual PDFДокумент71 страница1224 Threading Machine - Operator's Manual PDFAlberto Flores FrancoОценок пока нет
- Piriformissyndrome Exercise Sheet PDFДокумент2 страницыPiriformissyndrome Exercise Sheet PDFherikОценок пока нет
- Chest TraumaДокумент115 страницChest TraumaЕвгений ХанькоОценок пока нет
- ComplaintДокумент5 страницComplaintShericka Jade MontorОценок пока нет
- TRM 409.01 "Ethics of Consumer Production and Marketing"Документ4 страницыTRM 409.01 "Ethics of Consumer Production and Marketing"Neşe RomanОценок пока нет
- The Paper Doctor TEXTOДокумент101 страницаThe Paper Doctor TEXTOondasdeforma67% (3)
- Sorbion SachetsДокумент3 страницыSorbion SachetsReil_InsulaОценок пока нет
- Basic Machine Training GuideДокумент22 страницыBasic Machine Training GuideFernando Lopez CamposОценок пока нет
- Shoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaДокумент11 страницShoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaAbyudya Rafif KurniawanОценок пока нет
- Shock Study Guide NursingДокумент4 страницыShock Study Guide NursingKory Christina100% (2)
- Pedal Cycle Helmet Position Paper FinalДокумент2 страницыPedal Cycle Helmet Position Paper FinaljusendqОценок пока нет
- Case Present AclДокумент60 страницCase Present AclNovell VeliaОценок пока нет
- 08-12-2019 (20.30), Ch. Ivan, 14 Yo, Close Fraktur 1-3 Distal Os Radius Dextra, Dr. Tri Tuty H, SP - OtДокумент14 страниц08-12-2019 (20.30), Ch. Ivan, 14 Yo, Close Fraktur 1-3 Distal Os Radius Dextra, Dr. Tri Tuty H, SP - OtRa' DesireeОценок пока нет
- Pulp ProtectionДокумент4 страницыPulp ProtectionNaji Z. Arandi0% (1)
- ATI Med Surg SPRING 2019 Post ReviewДокумент11 страницATI Med Surg SPRING 2019 Post ReviewQuincey Hamilton43% (7)
- Vertebral Column Skull Projection MethodДокумент8 страницVertebral Column Skull Projection MethodLaFranz CabotajeОценок пока нет
- He2011 TMJ ANKYLOSIS CLASSIFICATIONДокумент8 страницHe2011 TMJ ANKYLOSIS CLASSIFICATIONPorcupine TreeОценок пока нет
- Tanduay DistillersДокумент8 страницTanduay DistillersAnna BautistaОценок пока нет
- Genesys Spell SummaryДокумент16 страницGenesys Spell SummaryxyliansnetworkОценок пока нет
- CAHB-20 Operating Manual enДокумент60 страницCAHB-20 Operating Manual enDavid Lay IIОценок пока нет
- START Triage Training Presentation TTT 8 31 - 1 PDFДокумент95 страницSTART Triage Training Presentation TTT 8 31 - 1 PDFCM NajitoОценок пока нет
- Stage Makeup2016 CompleteДокумент46 страницStage Makeup2016 Completeapi-319037565Оценок пока нет
- Fracture RehabilitationДокумент43 страницыFracture Rehabilitationnanahossam12345Оценок пока нет
- Sample Resolution On Frustrated MurderДокумент3 страницыSample Resolution On Frustrated MurderIrish LicoОценок пока нет
- List of Clotting FactorsДокумент3 страницыList of Clotting FactorsMa Cheryll DueñasОценок пока нет