Вам также может понравиться
- Ssri Presentation - 674 - Final2Документ52 страницыSsri Presentation - 674 - Final2api-289842236100% (1)
- Nutritional Treatments For Opioid AddictionДокумент4 страницыNutritional Treatments For Opioid AddictionEnzoОценок пока нет
- Pristiq (Desvenlafaxine) Product Monograph For CanadaДокумент48 страницPristiq (Desvenlafaxine) Product Monograph For CanadajennabushОценок пока нет
- Drugs of Abuse: Rita Dries Senior Lecturer KHK Turnhout - BelgiëДокумент32 страницыDrugs of Abuse: Rita Dries Senior Lecturer KHK Turnhout - BelgiëKartikОценок пока нет
- Stimulants: Jeremy LuoДокумент30 страницStimulants: Jeremy LuoJeremy LuoОценок пока нет
- Level 2 Depression AdultДокумент3 страницыLevel 2 Depression AdultwaleskacrzОценок пока нет
- A Presentation About DrugsДокумент18 страницA Presentation About Drugslaraesteban100% (1)
- SeroquelДокумент1 страницаSeroquelE100% (1)
- GHB PresentationДокумент19 страницGHB PresentationScorpion legionОценок пока нет
- Black Box WarningДокумент17 страницBlack Box WarningSantosh AdhikariОценок пока нет
- Mechanism of Action of QuetiapineДокумент4 страницыMechanism of Action of QuetiapineThoha AlbaarОценок пока нет
- Substance Use DisordersДокумент28 страницSubstance Use DisordersAbdul NazarОценок пока нет
- Psychoactive Drugs: The Proper Way of Using Drugs and What Effect It My Bring To UsДокумент14 страницPsychoactive Drugs: The Proper Way of Using Drugs and What Effect It My Bring To Usathena villaОценок пока нет
- Psychotropic MedicationsДокумент87 страницPsychotropic MedicationsDWAI McJohnsonОценок пока нет
- 8 Cns StimulantsДокумент46 страниц8 Cns StimulantslouradelОценок пока нет
- Detox OverviewДокумент6 страницDetox OverviewLauren EОценок пока нет
- Psychotropic Drugs: By: Rheajane Aguilar-RosalesДокумент77 страницPsychotropic Drugs: By: Rheajane Aguilar-Rosalesjean samson100% (1)
- Central Nervous System StimulantsДокумент20 страницCentral Nervous System StimulantsAn LoОценок пока нет
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsДокумент29 страницPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaОценок пока нет
- Mental Disorders and ComorbidityДокумент25 страницMental Disorders and ComorbidityFrida Neila RahmatikaОценок пока нет
- PSY1011 - Psychological Disorders LectureДокумент61 страницаPSY1011 - Psychological Disorders LectureeeОценок пока нет
- Gradual Dose Reduction ScheduleДокумент5 страницGradual Dose Reduction ScheduleAhmad Mujahid Huzaidi100% (1)
- Opioid PharmacologyДокумент47 страницOpioid PharmacologyEva K. Al KaryОценок пока нет
- Adrenergic Blocking, Cholinergic, Sedatives and Hypnotic WORDДокумент5 страницAdrenergic Blocking, Cholinergic, Sedatives and Hypnotic WORDKeon RicoОценок пока нет
- Dowden Health Media: For Personal Use OnlyДокумент8 страницDowden Health Media: For Personal Use OnlyfernandoОценок пока нет
- GP/Locum Drug List - 5 May 2013: RespiratoryДокумент14 страницGP/Locum Drug List - 5 May 2013: RespiratoryAdam ChungОценок пока нет
- Psychiatry Capstone 43020 Agitation PsychopharmacologyДокумент20 страницPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Оценок пока нет
- Role of Vitamin D in Schizophrenia in Elderly PatientДокумент3 страницыRole of Vitamin D in Schizophrenia in Elderly PatientJAVED ATHER SIDDIQUIОценок пока нет
- Depression: Types Symptoms Diagnosis Causes TreatmentДокумент32 страницыDepression: Types Symptoms Diagnosis Causes TreatmentThea MallariОценок пока нет
- CNS StimulantsДокумент89 страницCNS StimulantsMwanja Moses100% (1)
- Psychoactive DrugДокумент21 страницаPsychoactive DrugRagnar Jose RaskockОценок пока нет
- Initial Hospital Visit Inpatient Consult NoteДокумент6 страницInitial Hospital Visit Inpatient Consult NoteJanu easwarОценок пока нет
- Sedative-Hypnotics (SeH) and AnxiolyticsДокумент101 страницаSedative-Hypnotics (SeH) and Anxiolyticsmatchees-gone rogueОценок пока нет
- PrescriptionDrugsДокумент2 страницыPrescriptionDrugslosangelesОценок пока нет
- Guide To Harm Reduction ManualДокумент39 страницGuide To Harm Reduction ManualRaquelОценок пока нет
- AntideprresentДокумент54 страницыAntideprresentHadiqa KhanОценок пока нет
- Psychotropic DrugsДокумент60 страницPsychotropic DrugsLaTasha Lindemann RNОценок пока нет
- Substance Misuse Disorders: Dr. Ravi PaulДокумент19 страницSubstance Misuse Disorders: Dr. Ravi PaulRavi PaulОценок пока нет
- PA 644 - M2 LecturesДокумент735 страницPA 644 - M2 LectureskatОценок пока нет
- Stress Symptom Checklist: Physical Symptoms Psychological SymptomsДокумент1 страницаStress Symptom Checklist: Physical Symptoms Psychological Symptomsmaria pia otarolaОценок пока нет
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Документ3 страницыHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaОценок пока нет
- Drug Abuse, Addiction, and The BrainДокумент3 страницыDrug Abuse, Addiction, and The BrainArum ArysandiОценок пока нет
- Stimulant Use Disorder Assignment 2Документ15 страницStimulant Use Disorder Assignment 2Nathan MalamboОценок пока нет
- Drugsofabuse 190812163055 PDFДокумент28 страницDrugsofabuse 190812163055 PDFMargarita AmascualОценок пока нет
- Clinical Use of DexmedetomidineДокумент29 страницClinical Use of DexmedetomidineAnil SathyadasОценок пока нет
- The Effectiveness of Psychological Therapies On Drug Misusing ClientsДокумент16 страницThe Effectiveness of Psychological Therapies On Drug Misusing ClientsmargaridasolizОценок пока нет
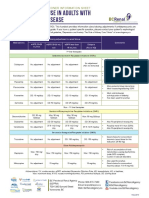
- Antidepressant Use in Adults With Chronic Kidney DiseaseДокумент1 страницаAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Treating and Beating Anxiety and DepressionДокумент7 страницTreating and Beating Anxiety and DepressiondrrodgermОценок пока нет
- Suicidal Ideation and Behavior in AdultsДокумент37 страницSuicidal Ideation and Behavior in AdultsAna Luz AlvarezОценок пока нет
- Substance Disorder 2020Документ59 страницSubstance Disorder 2020dennyzpsОценок пока нет
- General Questions (Mood Disorder)Документ5 страницGeneral Questions (Mood Disorder)Zubair MushtaqОценок пока нет
- Crestor PDFДокумент2 страницыCrestor PDFangelo017100% (1)
- PsychopharmacologyДокумент160 страницPsychopharmacologyInah Sarita100% (1)
- Psilocybin PPДокумент8 страницPsilocybin PPapi-532149591Оценок пока нет
- Dependence, Withdrawal and Rebound of CNSДокумент23 страницыDependence, Withdrawal and Rebound of CNSHassan AhmedОценок пока нет
- Prescribing BenzoДокумент10 страницPrescribing BenzoAndreea CraioveanuОценок пока нет
- Stop The Antipsychiatri C Medication: Done by Dr. Norah Al-Shatiri R3 Supervised by Dr. Kahled Al-JaberДокумент12 страницStop The Antipsychiatri C Medication: Done by Dr. Norah Al-Shatiri R3 Supervised by Dr. Kahled Al-JaberKhaled Al MadaniОценок пока нет
- Prescribing Guidelines For Benzodiazepines in Adults: BackgroundДокумент4 страницыPrescribing Guidelines For Benzodiazepines in Adults: BackgroundEfdio Manuel Joshiro SiagianОценок пока нет
- Chavez-Hernandez Et Al-2017-Suicide and Life-Threatening BehaviorДокумент6 страницChavez-Hernandez Et Al-2017-Suicide and Life-Threatening Behaviorlnair_43Оценок пока нет
- Comqol s5Документ55 страницComqol s5lnair_430% (1)
- VANCOUVER Reference Style Guide: NotesДокумент6 страницVANCOUVER Reference Style Guide: NotesMuhammad MoazzamОценок пока нет
- Developmental Needs of ChildrenДокумент3 страницыDevelopmental Needs of ChildrenTao WuОценок пока нет
- Lesson 2 Academic Writing StyleДокумент23 страницыLesson 2 Academic Writing StyleDonnel AlexanderОценок пока нет
- Tecp 222 Health AssignmentДокумент11 страницTecp 222 Health Assignmentapi-330392489Оценок пока нет
- Stephen Karcher - Great Vessel Blog PostsДокумент60 страницStephen Karcher - Great Vessel Blog PostsKenneth AndersonОценок пока нет
- LES SampleДокумент14 страницLES SampleKshitij_Batra_9305Оценок пока нет
- Audit Question List For ISO 9001Документ21 страницаAudit Question List For ISO 9001David Phoa100% (2)
- Road-Map Table GroupДокумент2 страницыRoad-Map Table GroupRichard WokardОценок пока нет
- Realism in Mid, Dle March - Briam MM, MJ, NBMJN SwannДокумент31 страницаRealism in Mid, Dle March - Briam MM, MJ, NBMJN SwannprankiplayspranksОценок пока нет
- Personality & Consumer BehaviourДокумент27 страницPersonality & Consumer BehaviourArathy Vikram100% (1)
- Test Specification Table: CT110-3-3-BSMA Individual Assignment Page 1 of 5Документ5 страницTest Specification Table: CT110-3-3-BSMA Individual Assignment Page 1 of 5Hamid ArashОценок пока нет
- The Status and Challenges of Ethiopian Higher Education System and Its Contribution To Development Teshome YizengawДокумент19 страницThe Status and Challenges of Ethiopian Higher Education System and Its Contribution To Development Teshome YizengawMahedre ZenebeОценок пока нет
- Design For Instruction Sse 3312 Unit Plan Rev 2015Документ3 страницыDesign For Instruction Sse 3312 Unit Plan Rev 2015api-282411249Оценок пока нет
- Performance AppraisalДокумент17 страницPerformance Appraisalemmanuel nyakiОценок пока нет
- Iep Case StudyДокумент31 страницаIep Case Studyapi-273265436Оценок пока нет
- Adjective String Lesson PlanДокумент3 страницыAdjective String Lesson PlanandrewaweberОценок пока нет
- (SUNY Series in Philosophy) William Maker-Philosophy Without Foundations - Rethinking Hegel-State University of New York Press (1994)Документ329 страниц(SUNY Series in Philosophy) William Maker-Philosophy Without Foundations - Rethinking Hegel-State University of New York Press (1994)redolfiriva77Оценок пока нет
- Differences Between Summarizing and Synthesizing InformationДокумент2 страницыDifferences Between Summarizing and Synthesizing InformationDr. Sarah Elaine Eaton50% (4)
- 4 - 02-25-2021 - 16-19-14 - Master of Art 4th Sem (Only Re-Appear) Exams March, 2021Документ3 страницы4 - 02-25-2021 - 16-19-14 - Master of Art 4th Sem (Only Re-Appear) Exams March, 2021parteek 3636Оценок пока нет
- HPI GuidelinesДокумент5 страницHPI GuidelinesHani NadiahОценок пока нет
- Ogl 365 Final Project PaperДокумент9 страницOgl 365 Final Project Paperapi-624910201Оценок пока нет
- The 36 Roles - Genetic Continuity and Mastery of Lines (Ra Uru Hu) (Z-Library)Документ76 страницThe 36 Roles - Genetic Continuity and Mastery of Lines (Ra Uru Hu) (Z-Library)Yan Guangyuan100% (1)
- Sylvester Aggor: ObjectiveДокумент2 страницыSylvester Aggor: ObjectiveAnonymous zt1XakvzvОценок пока нет
- Module 4Документ64 страницыModule 4Jagadeswar Babu100% (1)
- Chess and Philosophy A Rational ConversaДокумент8 страницChess and Philosophy A Rational ConversaReza R. W. TehusalawanyОценок пока нет
- Criminal Sociology Q&a Part IiiДокумент10 страницCriminal Sociology Q&a Part IiiDonita BernardinoОценок пока нет
- Sample Proposal DummyДокумент8 страницSample Proposal DummyArifur Rahman HeraОценок пока нет
- Speaking Questions For The First SemesterДокумент2 страницыSpeaking Questions For The First SemesterTrâm NguyễnОценок пока нет
- English Club AMSAДокумент2 страницыEnglish Club AMSAIntan Karnina PutriОценок пока нет
- Consumers' Perception Towards Online Shopping: A Case Study On Malaysian MarketДокумент12 страницConsumers' Perception Towards Online Shopping: A Case Study On Malaysian MarketPuteri IzzgОценок пока нет
- Written Works On Ma'am LumbuanДокумент3 страницыWritten Works On Ma'am LumbuanJAYSON GARGARITANOОценок пока нет
- Psychology Project 2016-2017: The Indian Community School, KuwaitДокумент21 страницаPsychology Project 2016-2017: The Indian Community School, KuwaitnadirkadhijaОценок пока нет