Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Five Element PointsДокумент42 страницыFive Element PointsSundar Rajan78% (9)
- History Taking in JaundiceДокумент2 страницыHistory Taking in Jaundiceshanyiar100% (5)
- Dimensional Modeling Basics For HealthcareДокумент27 страницDimensional Modeling Basics For Healthcareduwayne_willettОценок пока нет
- CefepimeДокумент2 страницыCefepimeMae Ann Bueno CastillonОценок пока нет
- 3M Slide - CHG Dressing For CRBSI (Juli 2022)Документ20 страниц3M Slide - CHG Dressing For CRBSI (Juli 2022)SilviyhaОценок пока нет
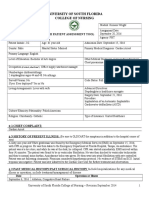
- Pat Fundamentals of Nursing PracticeДокумент22 страницыPat Fundamentals of Nursing Practiceapi-365123958Оценок пока нет
- Pat 2 Med Surg IIДокумент28 страницPat 2 Med Surg IIapi-365123958Оценок пока нет
- Quality and Safety Sythesis PresentationДокумент9 страницQuality and Safety Sythesis Presentationapi-365123958Оценок пока нет
- Pat 2 Med Surg IДокумент27 страницPat 2 Med Surg Iapi-365123958Оценок пока нет
- DR JordanДокумент7 страницDR Jordanapi-365123958Оценок пока нет
- Pat 1 Med Surg IIДокумент31 страницаPat 1 Med Surg IIapi-365123958Оценок пока нет
- Community Health Capstone Paper - Children Living in Poverty in Broward CountyДокумент14 страницCommunity Health Capstone Paper - Children Living in Poverty in Broward Countyapi-365123958Оценок пока нет
- NpwsДокумент4 страницыNpwsapi-365123958Оценок пока нет
- Preceptor EvaluationДокумент1 страницаPreceptor Evaluationapi-365123958Оценок пока нет
- Synthesis PaperДокумент10 страницSynthesis Paperapi-365123958Оценок пока нет
- Pat Fundamentals of Nursing PracticeДокумент22 страницыPat Fundamentals of Nursing Practiceapi-365123958Оценок пока нет
- Nutrition Assessment-Congestive Heart FailureДокумент4 страницыNutrition Assessment-Congestive Heart Failureapi-365123958100% (1)
- Ta 102 Improving Health EquityДокумент1 страницаTa 102 Improving Health Equityapi-365123958Оценок пока нет
- Pat 2 Med Surg IIДокумент28 страницPat 2 Med Surg IIapi-365123958Оценок пока нет
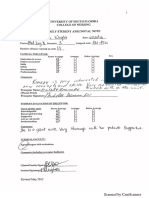
- Daily Anecdotal NotesДокумент6 страницDaily Anecdotal Notesapi-365123958Оценок пока нет
- Citi Module-Biomedical Biomed Investigators and Key Personnel Module-1Документ1 страницаCiti Module-Biomedical Biomed Investigators and Key Personnel Module-1api-365123958Оценок пока нет
- Pharmacotherapy of Smoking CessationДокумент1 страницаPharmacotherapy of Smoking Cessationapi-365123958Оценок пока нет
- Ta 101 Introduction To Population HealthДокумент1 страницаTa 101 Introduction To Population Healthapi-365123958Оценок пока нет
- Motivational Interviewing in Tobacco CessationДокумент1 страницаMotivational Interviewing in Tobacco Cessationapi-365123958Оценок пока нет
- Fema CertificateДокумент1 страницаFema Certificateapi-365123958Оценок пока нет
- Belle Witter Elementary School Certificate of AppreciationДокумент1 страницаBelle Witter Elementary School Certificate of Appreciationapi-365123958Оценок пока нет
- Personal Achievement AwardДокумент1 страницаPersonal Achievement Awardapi-365123958Оценок пока нет
- Stti Honor Society of NursingДокумент1 страницаStti Honor Society of Nursingapi-365123958Оценок пока нет
- Lutheran Social Services Certificate of AppreciationДокумент1 страницаLutheran Social Services Certificate of Appreciationapi-365123958Оценок пока нет
- Usf Certificate of AppreciationДокумент1 страницаUsf Certificate of Appreciationapi-365123958Оценок пока нет
- Kimone Wright - Registered Nurse ResumeДокумент2 страницыKimone Wright - Registered Nurse Resumeapi-365123958Оценок пока нет
- Feeding Tampa BayДокумент1 страницаFeeding Tampa Bayapi-365123958Оценок пока нет
- Clinical ExemplarДокумент4 страницыClinical Exemplarapi-365123958Оценок пока нет
- Personal and Professional GoalsДокумент2 страницыPersonal and Professional Goalsapi-365123958Оценок пока нет
- Effect of Intravenous Pamidronate Treatment in Children With Osteogenesis ImperfectaДокумент5 страницEffect of Intravenous Pamidronate Treatment in Children With Osteogenesis Imperfectavikash singhОценок пока нет
- Army Medicine:: Maintaining, Restoring, and Improving HealthДокумент92 страницыArmy Medicine:: Maintaining, Restoring, and Improving HealthLeo Mak Hoi-fong100% (1)
- Severe Gastric ImpactionДокумент4 страницыSevere Gastric ImpactionNanda Ayu Cindy KashiwabaraОценок пока нет
- Pneumonia Vaccine For ChildrenДокумент1 страницаPneumonia Vaccine For ChildrenPrincess Gutierrez RositaОценок пока нет
- Benefits of Equality ToolkitДокумент64 страницыBenefits of Equality ToolkitBasic Rights OregonОценок пока нет
- Annexure 'CD - 01' FORMAT FOR COURSE CURRICULUMДокумент4 страницыAnnexure 'CD - 01' FORMAT FOR COURSE CURRICULUMYash TiwariОценок пока нет
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsДокумент2 страницыNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comОценок пока нет
- Multiple Births Definition, Causes & CareДокумент11 страницMultiple Births Definition, Causes & CareCacing UcilОценок пока нет
- CaseДокумент31 страницаCaseErnes PutraОценок пока нет
- Furunculosis: Pathology Diagnosis Aetiology Outcomes Management OptionsДокумент2 страницыFurunculosis: Pathology Diagnosis Aetiology Outcomes Management OptionsGirish SubashОценок пока нет
- Pharmacoeconomics - Part IIIДокумент29 страницPharmacoeconomics - Part IIISima JabbariОценок пока нет
- AYR Patient Experience PresentationДокумент29 страницAYR Patient Experience Presentationaustin_tx6Оценок пока нет
- Pharyngitis Laryngitis TonsillitisДокумент10 страницPharyngitis Laryngitis Tonsillitisapi-457923289Оценок пока нет
- Atlantis Implant Compatibility Chart 79214-US-1107Документ2 страницыAtlantis Implant Compatibility Chart 79214-US-1107Jean-Christophe PopeОценок пока нет
- MRI Monitoring System Provides Safety and MobilityДокумент4 страницыMRI Monitoring System Provides Safety and MobilityAchiyat WinataОценок пока нет
- Medication - ALT-Template - Docusate SodiumДокумент1 страницаMedication - ALT-Template - Docusate SodiumNancyAmissahОценок пока нет
- Drug Card LansinohДокумент2 страницыDrug Card LansinohAdrianne Bazo100% (2)
- Ross University 2010-2011 Pre-Residency Planning GuideДокумент61 страницаRoss University 2010-2011 Pre-Residency Planning GuidescatteredbrainОценок пока нет
- Fatal Airway Obstruction Due To Ludwig'sДокумент6 страницFatal Airway Obstruction Due To Ludwig'sRegina MugopalОценок пока нет
- BSP Price List Agustus 2020Документ46 страницBSP Price List Agustus 2020Anonymous aaAQ6dgОценок пока нет
- Concept Map Draft ExampleДокумент2 страницыConcept Map Draft ExamplemeliОценок пока нет
- Daftar Obat High AlertДокумент2 страницыDaftar Obat High Alertayu aОценок пока нет
- AutohalerДокумент51 страницаAutohalerLinto JohnОценок пока нет
- Case StudyДокумент5 страницCase StudyHomework PingОценок пока нет