Вам также может понравиться
- Inhaled Salbutamol Plus Ipratropium in Moderate and Severe AsthmaДокумент6 страницInhaled Salbutamol Plus Ipratropium in Moderate and Severe AsthmaAriОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Anemia Anak 2: Dr. BerthaДокумент35 страницAnemia Anak 2: Dr. BerthaAriОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Daftar Isi PulmoДокумент5 страницDaftar Isi PulmoAriОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- JpedsДокумент7 страницJpedsAriОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Meta-Analysis of The Efficacy of A Single Dose of Phenylephrine 10mg Compared With Placebo in Adults With Acute Nasal Congestion Due To The Common ColdДокумент14 страницMeta-Analysis of The Efficacy of A Single Dose of Phenylephrine 10mg Compared With Placebo in Adults With Acute Nasal Congestion Due To The Common ColdAriОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Absorption and Fluoresence Spectra of Methyl Salicylate in The Vapor PhaseДокумент7 страницAbsorption and Fluoresence Spectra of Methyl Salicylate in The Vapor PhaseAriОценок пока нет
- Bmri2014 606021Документ11 страницBmri2014 606021AriОценок пока нет
- Evaluation of Step-Down Therapy From An Inhaled Steroid To Montelukast in Childhood AsthmaДокумент7 страницEvaluation of Step-Down Therapy From An Inhaled Steroid To Montelukast in Childhood AsthmaAriОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Essential Oils in The Treatment of Respiratory Tract Diseases Highlighting Their Role in Bacterial Infections and Their Anti-Inflammatory Action: A ReviewДокумент11 страницEssential Oils in The Treatment of Respiratory Tract Diseases Highlighting Their Role in Bacterial Infections and Their Anti-Inflammatory Action: A ReviewAri100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Pharmacologic Agents For Chronic DiarrheaДокумент7 страницPharmacologic Agents For Chronic DiarrheaAriОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Determining Cancer Survivors' Preferences To Inform New Models of Follow Up CareДокумент9 страницDetermining Cancer Survivors' Preferences To Inform New Models of Follow Up CareAriОценок пока нет
- Use of Oral Gentamicin, Metronidazole, and Cholestyramine in The Treatment of Severe Persistent Diarrhea in InfantsДокумент7 страницUse of Oral Gentamicin, Metronidazole, and Cholestyramine in The Treatment of Severe Persistent Diarrhea in InfantsAriОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- 197-2007 Woolcock Peak Flow ChartДокумент2 страницы197-2007 Woolcock Peak Flow ChartChow Sing SingОценок пока нет
- Critical Appraisal 'Prognosis'Документ27 страницCritical Appraisal 'Prognosis'Rizky Indah SorayaОценок пока нет
- Tindakan TorakosentesisДокумент15 страницTindakan TorakosentesisAyu Ayu AyuОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Tahitian Noni Juice Clinical TrialsДокумент1 страницаTahitian Noni Juice Clinical TrialsEd50% (2)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Atropine Treatment 1Документ7 страницAtropine Treatment 1Chris ChowОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- PfizerДокумент10 страницPfizerNayan ShuklaОценок пока нет
- Asthma QOLДокумент7 страницAsthma QOLjastevensonОценок пока нет
- Intergroup Phase III RCT On Unresectable Head and Neck CancersДокумент7 страницIntergroup Phase III RCT On Unresectable Head and Neck CancersjmbobitОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Glickman (1) - Ethical and Scientific Implications of The Globalization of Clinical Research NEJMДокумент8 страницGlickman (1) - Ethical and Scientific Implications of The Globalization of Clinical Research NEJMMaria BernalОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- HomeopathyДокумент50 страницHomeopathyArpita Mishra100% (1)
- Medical Technology CoursesДокумент3 страницыMedical Technology CoursesAly Bint SmbsОценок пока нет
- Delamanid For MDR TB (Journal Reading)Документ20 страницDelamanid For MDR TB (Journal Reading)Gede Ngurah ProboОценок пока нет
- Clean Versus Sterile Management of Chronic WoundsДокумент3 страницыClean Versus Sterile Management of Chronic WoundsDon RicaforteОценок пока нет
- Leong 2019Документ10 страницLeong 2019David UriosteguiОценок пока нет
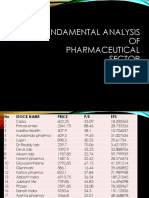
- Fundamental Analysis of Pharmaceutical SectorДокумент10 страницFundamental Analysis of Pharmaceutical SectorHarsh parasher (PGDM 17-19)Оценок пока нет
- Daftar BukuДокумент30 страницDaftar BukuRezeki AdnaveОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Acute Ankle Sprain - An UpdateДокумент7 страницAcute Ankle Sprain - An UpdateFran Leiva CorreaОценок пока нет
- Insomnia and CanabisДокумент10 страницInsomnia and CanabisEbetWasuwayОценок пока нет
- Final ReportДокумент53 страницыFinal ReportParth Gandhi100% (1)
- Sample Consent FormДокумент15 страницSample Consent FormSi Hacin AkoОценок пока нет
- Abbott LaboratoriesДокумент6 страницAbbott LaboratoriesdineshkoriОценок пока нет
- Parachute Use To Prevent Death and Major Trauma When Jumping From Aircraft: Randomized Controlled TrialДокумент6 страницParachute Use To Prevent Death and Major Trauma When Jumping From Aircraft: Randomized Controlled TrialAlexandre Campos Moraes AmatoОценок пока нет
- Wurzel 2016Документ8 страницWurzel 2016prolanis pkmmulyoharjoОценок пока нет
- Tea TreeДокумент4 страницыTea TreeRakeshKumarОценок пока нет
- Tuitu 15.6.2014Документ4 страницыTuitu 15.6.2014RimenhawihiОценок пока нет
- Notice: Meetings: National Institute of Neurological Disorders and StrokeДокумент1 страницаNotice: Meetings: National Institute of Neurological Disorders and StrokeJustia.comОценок пока нет
- STD 12 Science Group B Ready Recknor VДокумент36 страницSTD 12 Science Group B Ready Recknor Vfree accag100% (2)
- نموذج طلب إضافة أو حذف دواء للمرشد الطبي العلاجي الوطنيДокумент4 страницыنموذج طلب إضافة أو حذف دواء للمرشد الطبي العلاجي الوطنيSamer KhalladОценок пока нет
- Jurna NuromolДокумент6 страницJurna NuromolFriedrick VecchioОценок пока нет
- Chapter 3 Rationality of DrugsДокумент56 страницChapter 3 Rationality of DrugsS.Srinivasan ('Chinu'); Renu KhannaОценок пока нет