Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Surviving Chemistry: A Guided Study Book For High School ChemistryДокумент83 страницыSurviving Chemistry: A Guided Study Book For High School ChemistryE3 Scholastic Publishing100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Color Atlas of EndoДокумент203 страницыColor Atlas of Endooana_en100% (23)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Pavement DesignДокумент598 страницPavement Designaby_abraham5005100% (4)
- Coagulation FlocculationДокумент71 страницаCoagulation FlocculationDeepa Singh100% (1)
- Prosthodontics in Clinical Practice PDFДокумент232 страницыProsthodontics in Clinical Practice PDFanastoma100% (1)
- Prosthodontics in Clinical Practice PDFДокумент232 страницыProsthodontics in Clinical Practice PDFanastoma100% (1)
- Illuminating The Path To EnlightenmentДокумент125 страницIlluminating The Path To Enlightenmentanastoma100% (2)
- DP Test ProcedureДокумент8 страницDP Test ProcedureAjith KumarОценок пока нет
- KAESER SX6 Service ManualДокумент100 страницKAESER SX6 Service ManualYassin AlkadyОценок пока нет
- Sample Problem #1Документ7 страницSample Problem #1DozdiОценок пока нет
- Tutorial Chapter 02 - AnswerДокумент8 страницTutorial Chapter 02 - AnswerFateh Hakeem100% (4)
- Current Concepts and Techniques For Caries Excavation and Adhesion To Residual Dentin, J Adhesi Dent 2011Документ17 страницCurrent Concepts and Techniques For Caries Excavation and Adhesion To Residual Dentin, J Adhesi Dent 2011Jesus NavarreteОценок пока нет
- 39.4 01 Evidence-Based Update Restorative 2 FINALДокумент9 страниц39.4 01 Evidence-Based Update Restorative 2 FINALanastomaОценок пока нет
- Albirea Dintilor Vitali PDFДокумент8 страницAlbirea Dintilor Vitali PDFanastomaОценок пока нет
- Articol CimentareДокумент7 страницArticol CimentareanastomaОценок пока нет
- Curs 2017 UPBДокумент78 страницCurs 2017 UPBanastomaОценок пока нет
- Safety Data Sheet: 1 IdentificationДокумент16 страницSafety Data Sheet: 1 IdentificationanastomaОценок пока нет
- Curs 2017 UPBДокумент78 страницCurs 2017 UPBanastomaОценок пока нет
- Intracanal Medicament in Pediatric EndodonticsДокумент6 страницIntracanal Medicament in Pediatric EndodonticsVilianti Eka Fitri RahatinaОценок пока нет
- Fracture Resistance of Teeth Restored With All-Ceramic Inlays and Onlays: An in Vitro StudyДокумент9 страницFracture Resistance of Teeth Restored With All-Ceramic Inlays and Onlays: An in Vitro StudyMarta BabiiОценок пока нет
- Fracture Resistance of Teeth Restored With All-Ceramic Inlays and Onlays: An in Vitro StudyДокумент9 страницFracture Resistance of Teeth Restored With All-Ceramic Inlays and Onlays: An in Vitro StudyMarta BabiiОценок пока нет
- Discussion On How Alice Munro Establishes Mood Atmosphere and Relationships in The Exposition of Postcard 15Документ3 страницыDiscussion On How Alice Munro Establishes Mood Atmosphere and Relationships in The Exposition of Postcard 15anastomaОценок пока нет
- Microsoft Powerpoint - Tooth Colored Inlays and Onlays - IДокумент53 страницыMicrosoft Powerpoint - Tooth Colored Inlays and Onlays - Ianastoma100% (1)
- Patologie Orala Curs 2Документ34 страницыPatologie Orala Curs 2anastomaОценок пока нет
- Urgente in EndodontieДокумент2 страницыUrgente in EndodontieanastomaОценок пока нет
- Blue Bloods 1Документ166 страницBlue Bloods 1anastomaОценок пока нет
- Patologie Orala Curs 2Документ34 страницыPatologie Orala Curs 2anastomaОценок пока нет
- Reabilitare-DVO Curs 2Документ34 страницыReabilitare-DVO Curs 2anastomaОценок пока нет
- Reabilitare Orala C120130416103143640Документ49 страницReabilitare Orala C120130416103143640anastomaОценок пока нет
- Albirea Dintilor Vitali PDFДокумент8 страницAlbirea Dintilor Vitali PDFanastomaОценок пока нет
- Reabilirare C320130416103133333Документ22 страницыReabilirare C320130416103133333anastomaОценок пока нет
- Patologie Orala Curs 2Документ34 страницыPatologie Orala Curs 2anastomaОценок пока нет
- PDQ Endodontic, IntroductionДокумент14 страницPDQ Endodontic, Introductiondent in dentistОценок пока нет
- Albirea Dintilor Vitali PDFДокумент8 страницAlbirea Dintilor Vitali PDFanastomaОценок пока нет
- Bridges PDFДокумент48 страницBridges PDFanastomaОценок пока нет
- 100 de Personal It A Ti - EinsteinДокумент32 страницы100 de Personal It A Ti - Einsteinsheikare100% (1)
- 1 s2.0 S0048969721053572 MainДокумент15 страниц1 s2.0 S0048969721053572 MainMakhitha MasipaОценок пока нет
- European Copper Institute European Copper Institute: Architectural ApplicationsДокумент52 страницыEuropean Copper Institute European Copper Institute: Architectural ApplicationsstankoubОценок пока нет
- Checklist To Design AssembliesДокумент1 страницаChecklist To Design AssembliesRobert GalarzaОценок пока нет
- High Voltage Transformer: InstructablesДокумент6 страницHigh Voltage Transformer: InstructablespinoОценок пока нет
- TitaniumДокумент6 страницTitaniumzonearthОценок пока нет
- FCU Link V2 CatalogueДокумент17 страницFCU Link V2 CatalogueVipul JainОценок пока нет
- Hall Sensors Selection GuideДокумент2 страницыHall Sensors Selection GuideMiltongrimi GrimilОценок пока нет
- Gear Reference PDFДокумент15 страницGear Reference PDFXuan Phuong HuynhОценок пока нет
- Sheet Rolling Machine - SynopsisДокумент8 страницSheet Rolling Machine - SynopsisTanviОценок пока нет
- Identify The Following: Cien 3090 Construction Materials & Testing Midterm ExamДокумент1 страницаIdentify The Following: Cien 3090 Construction Materials & Testing Midterm Examacurvz2005Оценок пока нет
- Akay Acoustics of Friction PDFДокумент24 страницыAkay Acoustics of Friction PDFgene_sparcОценок пока нет
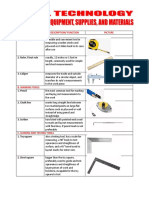
- Tool/ Equipment Description/ Function Picture A. Measuring ToolsДокумент13 страницTool/ Equipment Description/ Function Picture A. Measuring ToolsNicolas AntiguaОценок пока нет
- 1.1 System Overview 1.2 FunctionДокумент8 страниц1.1 System Overview 1.2 FunctionNwachukwu UmehОценок пока нет
- n7k ReplacingДокумент102 страницыn7k ReplacingMcyanogen HeshamОценок пока нет
- Nano MaterialsДокумент252 страницыNano MaterialsSms RajaОценок пока нет
- Final Canvass PDFДокумент3 страницыFinal Canvass PDFjavierb.jungОценок пока нет
- FLOWTITE - Installation Guide For Buried Pipes - AWWA - Abbr. Version - enДокумент31 страницаFLOWTITE - Installation Guide For Buried Pipes - AWWA - Abbr. Version - envuqar0979Оценок пока нет
- GPT 1-3 PGE Tech SpecificationsДокумент4 страницыGPT 1-3 PGE Tech SpecificationsEhtisham AndrAbiОценок пока нет
- Datasheet RefDem58219080-3400-30 en 120V 60Hz-2Документ7 страницDatasheet RefDem58219080-3400-30 en 120V 60Hz-2Floyd PriceОценок пока нет
- Water Treatment Presentation (WEMCO vs. Enviro-Cell) .PPSXДокумент18 страницWater Treatment Presentation (WEMCO vs. Enviro-Cell) .PPSXJUAN PABLO RUIZ LARAОценок пока нет
- Materials Chemistry and Physics: Jure Zigon, Matja Z Pavli C, Marko Petri C, Sebastian DahleДокумент12 страницMaterials Chemistry and Physics: Jure Zigon, Matja Z Pavli C, Marko Petri C, Sebastian DahleAromoОценок пока нет
- Powder 1Документ84 страницыPowder 1Nyanda MadiliОценок пока нет
- Thermoplastic - WikipediaДокумент5 страницThermoplastic - Wikipediakirthi83Оценок пока нет