Вам также может понравиться
- Risk Management PlanДокумент2 страницыRisk Management Planrojon pharmacy84% (37)
- Pharmacology Notes (Chapter 20 and 21)Документ2 страницыPharmacology Notes (Chapter 20 and 21)graycorypОценок пока нет
- SNS and PNS Drugs (Cholinergics and Adrenergics)Документ5 страницSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- ADR Reporting FormДокумент2 страницыADR Reporting FormApoorva Tatti100% (1)
- Pharm Expansion 17 NDFДокумент1 страницаPharm Expansion 17 NDFNokz M. Raki-inОценок пока нет
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DДокумент28 страницAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaОценок пока нет
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDДокумент1 страницаCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiОценок пока нет
- Drugs in Blood DisordersДокумент1 страницаDrugs in Blood DisordersSantosh patelОценок пока нет
- PG PREPARATION - Mnemonics in PharmacologyДокумент12 страницPG PREPARATION - Mnemonics in PharmacologyRaveen KumarОценок пока нет
- Hierarchy of O2 Delivery SystemsДокумент1 страницаHierarchy of O2 Delivery SystemsRevОценок пока нет
- Drug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsДокумент7 страницDrug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsJenny NguyenОценок пока нет
- Adrenergic Receptor ChartДокумент1 страницаAdrenergic Receptor Chartsas345sas345Оценок пока нет
- Anticoagulants Drug TableДокумент1 страницаAnticoagulants Drug TableNicole HoОценок пока нет
- Common Prefixes and SuffixesДокумент5 страницCommon Prefixes and Suffixestriddle1969100% (1)
- Transport of Critically Ill Adults 2011Документ1 страницаTransport of Critically Ill Adults 2011velocity25Оценок пока нет
- Therapeutic IndexДокумент8 страницTherapeutic IndexMary Jennel RosОценок пока нет
- Pharmacology Main DrugsДокумент14 страницPharmacology Main DrugsSabir KhanОценок пока нет
- Administering Vaccines To AdultsДокумент1 страницаAdministering Vaccines To AdultsPaul Anthony LoricaОценок пока нет
- GI Motility DrugsДокумент1 страницаGI Motility DrugspulmonologistОценок пока нет
- Pharmacology A - NSAIDSДокумент14 страницPharmacology A - NSAIDSselflessdoctorОценок пока нет
- Renal Guide and Charts: AlbuminДокумент16 страницRenal Guide and Charts: AlbuminYaima JimenezОценок пока нет
- Common Asthma MedicationsДокумент1 страницаCommon Asthma MedicationsHeart of the Valley, Pediatric CardiologyОценок пока нет
- Labs Electrolyte ChartДокумент1 страницаLabs Electrolyte ChartmdcmepОценок пока нет
- Disorders of The BoneДокумент2 страницыDisorders of The BoneRPh Krishna Chandra JagritОценок пока нет
- Dka Guidelines - 2012Документ4 страницыDka Guidelines - 2012djizhieeОценок пока нет
- EAR First AidДокумент4 страницыEAR First Aidr_lakshmi2722Оценок пока нет
- Angina Pharmacology YeahДокумент16 страницAngina Pharmacology YeahMuhammad AfifuddinОценок пока нет
- Drug CardsДокумент3 страницыDrug CardsDave HillОценок пока нет
- Cardiovascular Nursing: Study Online atДокумент7 страницCardiovascular Nursing: Study Online atLilly DayeОценок пока нет
- Semester 2 Drug ListДокумент7 страницSemester 2 Drug ListNam_Pham_6481Оценок пока нет
- Milrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1Документ1 страницаMilrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1njones33Оценок пока нет
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsДокумент17 страницWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuОценок пока нет
- Critical Care Drugs 1Документ21 страницаCritical Care Drugs 1Asri ErnadiОценок пока нет
- Beta BlockersДокумент1 страницаBeta BlockersShrikant ThakurОценок пока нет
- Blank Physical Assessment SheetДокумент2 страницыBlank Physical Assessment SheetRenee Hickman RobinsonОценок пока нет
- Drug Classes and Brand NamesДокумент6 страницDrug Classes and Brand Namesremyde07Оценок пока нет
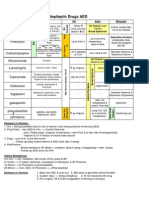
- Antiepileptic Drugs AED: D' DI Disadv SE AdvДокумент1 страницаAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Оценок пока нет
- Table of Sedative, Hypnotic, AntianxietyДокумент4 страницыTable of Sedative, Hypnotic, AntianxietyirfanzukriОценок пока нет
- MPIL2 Medical Professionals Guide To POTSJWДокумент12 страницMPIL2 Medical Professionals Guide To POTSJWAttis PhrygiaОценок пока нет
- Antiseizure, Sedative & HypnoticsДокумент8 страницAntiseizure, Sedative & HypnoticsThulasi tootsieОценок пока нет
- NHS Antibiotice PDFДокумент2 страницыNHS Antibiotice PDFHoratiu OanaОценок пока нет
- Pharmacology of Cardiac Diseases MINEДокумент3 страницыPharmacology of Cardiac Diseases MINEMitu Miressa تОценок пока нет
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNДокумент43 страницыNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- OS217 LEC06 Rational Antibiotic UseДокумент6 страницOS217 LEC06 Rational Antibiotic Usegenerics54321Оценок пока нет
- Bot Med Final CHARTДокумент33 страницыBot Med Final CHARTapi-26938624100% (3)
- Bam Slam Drug CardДокумент4 страницыBam Slam Drug CardLeticia GonzalezОценок пока нет
- Cheat Sheet For Fluid Balance and ElectrolytesДокумент2 страницыCheat Sheet For Fluid Balance and ElectrolytesLiel TorresОценок пока нет
- Adrenergic PharmacologyДокумент6 страницAdrenergic Pharmacologyjess6001Оценок пока нет
- Drug Compatibility in Intravenous Y-Site AdministrationДокумент4 страницыDrug Compatibility in Intravenous Y-Site Administrationtuti haryatiОценок пока нет
- Renal Excretion of DrugsДокумент3 страницыRenal Excretion of DrugsGerardLum100% (3)
- Insulin Chart 05032012 PDFДокумент1 страницаInsulin Chart 05032012 PDFTiffany CrittendenОценок пока нет
- Ninja - Anemias PDFДокумент1 страницаNinja - Anemias PDFErica Hyeyeon LeeОценок пока нет
- Abg InterpretationДокумент1 страницаAbg InterpretationPrincess EspadaОценок пока нет
- Agents Used in Cardiac ArrhythmiasДокумент4 страницыAgents Used in Cardiac ArrhythmiasKaye PatriaОценок пока нет
- NOAC ChartДокумент2 страницыNOAC Chartsgod34Оценок пока нет
- Parenting Styles: - Dictatorial or AuthoritarianДокумент45 страницParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningОценок пока нет
- Gout DrugsДокумент1 страницаGout DrugsMichael BrownОценок пока нет
- Nephrotic and NephriticДокумент27 страницNephrotic and Nephritictam meiОценок пока нет
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Drug StudyДокумент2 страницыDrug StudyemmanuelmyagokayeОценок пока нет
- Hypertensive CrisisДокумент1 страницаHypertensive Crisisapi-495201002Оценок пока нет
- RKNLKNKL 255Документ2 страницыRKNLKNKL 255Adam AdamakoОценок пока нет
- ApotekДокумент36 страницApotekyuka nagisaОценок пока нет
- AP Agung SerdamДокумент220 страницAP Agung Serdamjihan.luthfiyahОценок пока нет
- Laporan Stock All Principal 27 Desember 2021 Ams PDGДокумент52 страницыLaporan Stock All Principal 27 Desember 2021 Ams PDGVonny NoviaОценок пока нет
- Ultiva (Remifentanil) Side Effects, Interactions, Warning, Dosage & Uses PDFДокумент1 страницаUltiva (Remifentanil) Side Effects, Interactions, Warning, Dosage & Uses PDFcarlnoinОценок пока нет
- Drug Therapy Assessment Worksheet (Dtaw)Документ5 страницDrug Therapy Assessment Worksheet (Dtaw)Mica Charish VillaluzОценок пока нет
- Tablets: RPH Saba Inayat Ali Lecturer Dcop DuhsДокумент77 страницTablets: RPH Saba Inayat Ali Lecturer Dcop Duhssaad najОценок пока нет
- GI Pharmacology QuestionsДокумент2 страницыGI Pharmacology QuestionsnassaglobalОценок пока нет
- Daftar Obat EthicalДокумент11 страницDaftar Obat EthicalhusnulОценок пока нет
- Danh Muc San Pham DHG 2016Документ60 страницDanh Muc San Pham DHG 2016Thư PhùngОценок пока нет
- Pharmaceutical Development: Lynda PaleshnuikДокумент57 страницPharmaceutical Development: Lynda PaleshnuikhuynhvinhquangОценок пока нет
- Label Kotak Obat BaruДокумент25 страницLabel Kotak Obat BaruOrin Tri WulanОценок пока нет
- Daftar Harga Obat Manfar 2020Документ14 страницDaftar Harga Obat Manfar 2020Novita YulianiОценок пока нет
- Pharma Unit 1-2 Anti - Adrenergic DrugsДокумент21 страницаPharma Unit 1-2 Anti - Adrenergic DrugsMIbrahimОценок пока нет
- QB Poisoning Final...Документ31 страницаQB Poisoning Final...richard bolinaoОценок пока нет
- Daftar Isi Ebook Ujian ApotekerДокумент2 страницыDaftar Isi Ebook Ujian ApotekerFiqua Nurul Rafiqua SimsОценок пока нет
- Principles of Drug Therapy in Dentistry PDFДокумент163 страницыPrinciples of Drug Therapy in Dentistry PDFJetter LeeОценок пока нет
- Abbreviation of PharmacologyДокумент59 страницAbbreviation of PharmacologyMohamed Abo EmadОценок пока нет
- Forcadilla Medsurg Drug StudyДокумент12 страницForcadilla Medsurg Drug StudyKeir Mrls ForcadillaОценок пока нет
- Acne TreatmentДокумент15 страницAcne TreatmentSeptia Kurniaty100% (1)
- ORAL COVERAGE-CDI 107 Lesson 6-FINALДокумент26 страницORAL COVERAGE-CDI 107 Lesson 6-FINALJoebellОценок пока нет
- Journal Club Presentation: DR Waleed AhmadДокумент30 страницJournal Club Presentation: DR Waleed Ahmadkaram aliОценок пока нет
- Kuantitas Obat Tahun NewДокумент18 страницKuantitas Obat Tahun NewFathia Afriza KurniawatiОценок пока нет
- Eap - Dins - List 2Документ58 страницEap - Dins - List 2Jenny JeongОценок пока нет
- Stiff Person Syndrome and AnesthesiaДокумент15 страницStiff Person Syndrome and AnesthesiaFarhan AshrafОценок пока нет
- Ah Fs Classification With DrugsДокумент30 страницAh Fs Classification With DrugsIndah Dian Perdana PutriОценок пока нет