Вам также может понравиться
- Surgery of the Cranio-Vertebral JunctionОт EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreОценок пока нет
- Mature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportДокумент5 страницMature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportHaribabuBabuОценок пока нет
- 4837 4839 A Reddish Pulsatile Mass Beyond Tympanic Membrane Think Before ActДокумент3 страницы4837 4839 A Reddish Pulsatile Mass Beyond Tympanic Membrane Think Before ActAluОценок пока нет
- Jpn. J. Clin. Oncol.-2014-Xue-926-31 PDFДокумент6 страницJpn. J. Clin. Oncol.-2014-Xue-926-31 PDFKarina Mega WОценок пока нет
- 1 s2.0 S1010518216000652 Main PDFДокумент9 страниц1 s2.0 S1010518216000652 Main PDFRoberto AmayaОценок пока нет
- Recurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionДокумент5 страницRecurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionlalajanОценок пока нет
- Originalarticle Open AccessДокумент8 страницOriginalarticle Open Accessfarah moonОценок пока нет
- 2 5400160637227631067 PDFДокумент7 страниц2 5400160637227631067 PDFSiska HarapanОценок пока нет
- The Diagnostic and Etiological Contribution of Sectional Imaging in Deafness (About 80 Cases)Документ7 страницThe Diagnostic and Etiological Contribution of Sectional Imaging in Deafness (About 80 Cases)IJAR JOURNALОценок пока нет
- Cholestoma Debriment PDFДокумент5 страницCholestoma Debriment PDFChairiniFikryОценок пока нет
- Hemimegalencephaly: A Study of Abnormalities Occurring Outside The Involved HemisphereДокумент5 страницHemimegalencephaly: A Study of Abnormalities Occurring Outside The Involved Hemisphereapi-148100258Оценок пока нет
- (10920684 - Neurosurgical Focus) Multiple Spinal Extradural Arachnoid Cysts Occurring in A ChildДокумент4 страницы(10920684 - Neurosurgical Focus) Multiple Spinal Extradural Arachnoid Cysts Occurring in A ChildRafael Mujica OreОценок пока нет
- Three-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaДокумент3 страницыThree-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaAdarsh GhoshОценок пока нет
- Treatment of Vascular Malformations of The Mandible: A Description of 12 CasesДокумент5 страницTreatment of Vascular Malformations of The Mandible: A Description of 12 CasesneyhaaОценок пока нет
- Nervios Mediastino PDFДокумент5 страницNervios Mediastino PDFteratocitoОценок пока нет
- A Pictorial Essay of Middle Ear Pathology Correlating Temporal Bone CT and MRI With Archived Otoscopic PhotographsДокумент17 страницA Pictorial Essay of Middle Ear Pathology Correlating Temporal Bone CT and MRI With Archived Otoscopic PhotographsTeuku Ahmad HasanyОценок пока нет
- Osteopathia Striata With Cranial SclerosisДокумент5 страницOsteopathia Striata With Cranial SclerosisritvikОценок пока нет
- 1523 FullДокумент10 страниц1523 FullBuat TugasОценок пока нет
- American Journal of OtolaryngologyДокумент4 страницыAmerican Journal of OtolaryngologyDear Farah SielmaОценок пока нет
- Eguchi2019 Article VestibularSymptomsInAcuteHemisДокумент7 страницEguchi2019 Article VestibularSymptomsInAcuteHemisrakhmararaОценок пока нет
- Article IJCCS 129Документ4 страницыArticle IJCCS 129Ari FevriandiОценок пока нет
- Morphology of Cranial Sutures and RadiologicДокумент6 страницMorphology of Cranial Sutures and RadiologicEvans RodrigezОценок пока нет
- Middle and Posterior Fossa AspergillomaДокумент4 страницыMiddle and Posterior Fossa AspergillomamuhammadОценок пока нет
- Foramen Huschke PatologicoДокумент7 страницForamen Huschke PatologicoLM AdrianneОценок пока нет
- Idiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewДокумент10 страницIdiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewSelfa YunitaОценок пока нет
- 619 FullДокумент12 страниц619 FullashajangamОценок пока нет
- Mandibular Traumatic Peripheral Osteoma: A Case ReportДокумент5 страницMandibular Traumatic Peripheral Osteoma: A Case ReportrajtanniruОценок пока нет
- Kim 2009Документ5 страницKim 2009ĐàoQuỳnhNhưОценок пока нет
- Accepted Manuscript: 10.1016/j.jcms.2017.12.013Документ16 страницAccepted Manuscript: 10.1016/j.jcms.2017.12.013stoia_sebiОценок пока нет
- Ewing Sarcoma, Anatomie NR 1Документ5 страницEwing Sarcoma, Anatomie NR 1Ioana PelinОценок пока нет
- Lawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseДокумент4 страницыLawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseSourabh PatroОценок пока нет
- Romano Et Al 2020 Solitary Fibrous Tumor of The Deep Parotid GlandДокумент3 страницыRomano Et Al 2020 Solitary Fibrous Tumor of The Deep Parotid GlandReyes Ivan García CuevasОценок пока нет
- Large Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaДокумент3 страницыLarge Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaJaya PrabhaОценок пока нет
- Scrotal Ultrasound in AdultsДокумент17 страницScrotal Ultrasound in AdultsMagzОценок пока нет
- Evaluation of Dural Venous Sinuses and Con Uence of Sinuses Via MRI Venography: Anatomy, Anatomic Variations, and The Classification of VariationsДокумент7 страницEvaluation of Dural Venous Sinuses and Con Uence of Sinuses Via MRI Venography: Anatomy, Anatomic Variations, and The Classification of VariationsYulita MustikasariОценок пока нет
- Lesi 2.1Документ6 страницLesi 2.1Dwi Putro SetiyantomoОценок пока нет
- Medip, IJRMS-7729 OДокумент7 страницMedip, IJRMS-7729 ORagupathi MОценок пока нет
- Inomata 1998Документ3 страницыInomata 1998jahfdfgsdjad asdhsajhajdkОценок пока нет
- 405 2013 Article 2598Документ5 страниц405 2013 Article 2598M Shiddiq GhiffariОценок пока нет
- DR - Khaldoun Osteoid Osteoma Case ReportДокумент4 страницыDR - Khaldoun Osteoid Osteoma Case ReportcyberjaleelОценок пока нет
- Mucoceles of The Paranasal Sinuses:: MR Imaging With CT CorrelationДокумент6 страницMucoceles of The Paranasal Sinuses:: MR Imaging With CT CorrelationArifah GulamanisОценок пока нет
- Combined Treatment of Surgery and Sclerotherapy For Sinus PericraniiДокумент5 страницCombined Treatment of Surgery and Sclerotherapy For Sinus Pericranii相壮壮Оценок пока нет
- Sleeve Fracture of The Adult PatellaДокумент3 страницыSleeve Fracture of The Adult PatellaRadenMasKaerОценок пока нет
- Imaging Hearing LossДокумент20 страницImaging Hearing LossmenafabОценок пока нет
- The Thoracic Anterior Spinal Cord Adhesion SyndromeДокумент7 страницThe Thoracic Anterior Spinal Cord Adhesion Syndromepaulina_810100% (1)
- Carotid Body Tumor As A Cause of Stroke2016Документ4 страницыCarotid Body Tumor As A Cause of Stroke2016Nicolas RodriguezОценок пока нет
- Temporal Bone TraumaДокумент16 страницTemporal Bone Traumadafita4661Оценок пока нет
- Adobe Scan 12 Aug 2023Документ2 страницыAdobe Scan 12 Aug 2023Gowtham LОценок пока нет
- 678 FullДокумент5 страниц678 Fullakram socisseОценок пока нет
- Recent Advances in MRI in The Preoperative Assessment of Anorectal MalformationsДокумент11 страницRecent Advances in MRI in The Preoperative Assessment of Anorectal Malformationsessy gusning rantiОценок пока нет
- Caso Clinico Sp3Документ4 страницыCaso Clinico Sp3eduardoОценок пока нет
- Degenerative Disk Disease of The Cervical Spine: Spectrum of Imaging FindingsДокумент53 страницыDegenerative Disk Disease of The Cervical Spine: Spectrum of Imaging FindingsAbo Saif Al MosewyОценок пока нет
- Cholesteatoma of External Auditory CanalДокумент5 страницCholesteatoma of External Auditory CanallolОценок пока нет
- Article in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyДокумент6 страницArticle in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusОценок пока нет
- Diagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature ReviewДокумент9 страницDiagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature Reviewsolikin ikinОценок пока нет
- Articol ORLДокумент6 страницArticol ORLSabina BădilăОценок пока нет
- Usefulness of HounsfeldДокумент12 страницUsefulness of HounsfeldBeautiful-Pretty Happy-WealthyОценок пока нет
- Raval PDFДокумент5 страницRaval PDFdebby claudiОценок пока нет
- Case Report: A Rare Stapes AbnormalityДокумент4 страницыCase Report: A Rare Stapes AbnormalityCarolina UrrutiaОценок пока нет
- Meningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiДокумент6 страницMeningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiNityaОценок пока нет
- Jurnal Anak Fix PDFДокумент17 страницJurnal Anak Fix PDFrisda aulia putriОценок пока нет
- BMJ Open-2014-Sung PDFДокумент7 страницBMJ Open-2014-Sung PDFrisda aulia putriОценок пока нет
- Drug Doses 2017Документ127 страницDrug Doses 2017Yuliawati HarunaОценок пока нет
- Ethical ClearanceДокумент1 страницаEthical Clearancerisda aulia putriОценок пока нет
- The Effect of Rotavirus Vaccine On Diarrhoea Mortality: BackgroundДокумент7 страницThe Effect of Rotavirus Vaccine On Diarrhoea Mortality: Backgroundrisda aulia putriОценок пока нет
- Hasil Uji DeskriptifДокумент4 страницыHasil Uji Deskriptifrisda aulia putriОценок пока нет
- Full Text Jurnal LactobasilusДокумент10 страницFull Text Jurnal Lactobasilusrisda aulia putriОценок пока нет
- Blood PresureДокумент8 страницBlood Presurerisda aulia putriОценок пока нет
- Post Partum Depression PDFДокумент9 страницPost Partum Depression PDFrisda aulia putriОценок пока нет
- Thailand PDFДокумент6 страницThailand PDFrisda aulia putriОценок пока нет
- Post Partum DepressionДокумент17 страницPost Partum Depressionrisda aulia putriОценок пока нет
- 1.kasus Nyeri Punggung IДокумент7 страниц1.kasus Nyeri Punggung Irisda aulia putriОценок пока нет
- Cancer Screening by Primary Care Physicians PDFДокумент6 страницCancer Screening by Primary Care Physicians PDFrisda aulia putriОценок пока нет
- Cervical VertigoДокумент14 страницCervical Vertigopuntocom111Оценок пока нет
- Family Medicine Between West and EastДокумент1 страницаFamily Medicine Between West and Eastrisda aulia putriОценок пока нет
- Family Physician Enabling AttitudesДокумент8 страницFamily Physician Enabling Attitudesrisda aulia putriОценок пока нет
- 1.kasus Nyeri Punggung IДокумент7 страниц1.kasus Nyeri Punggung Irisda aulia putriОценок пока нет
- 05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFДокумент6 страниц05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFrisda aulia putriОценок пока нет
- Family Physician Enabling AttitudesДокумент8 страницFamily Physician Enabling Attitudesrisda aulia putriОценок пока нет
- 5342 9112 1 PBДокумент5 страниц5342 9112 1 PBrisda aulia putriОценок пока нет
- Struma Ovarii Presenting With Hashimoto 'S Thyroiditis: A Case ReportДокумент4 страницыStruma Ovarii Presenting With Hashimoto 'S Thyroiditis: A Case Reportrisda aulia putriОценок пока нет
- Adult Ascites EnhancedДокумент96 страницAdult Ascites EnhancedPutri Rafika ZahrahОценок пока нет
- Struma Ovarii Presenting With Hashimoto 'S Thyroiditis: A Case ReportДокумент4 страницыStruma Ovarii Presenting With Hashimoto 'S Thyroiditis: A Case Reportrisda aulia putriОценок пока нет
- OA PrevalenceofBacterialVaginosisДокумент6 страницOA PrevalenceofBacterialVaginosisrisda aulia putriОценок пока нет
- 229Документ10 страниц229Machlery KunОценок пока нет
- 8.11.08 Davis-Hovda. TB PleurisyДокумент13 страниц8.11.08 Davis-Hovda. TB Pleurisyrisda aulia putriОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakarisdaauliaputriОценок пока нет
- Jurding JedingДокумент8 страницJurding JedingbungagobeОценок пока нет
- Environmental HazardsДокумент19 страницEnvironmental HazardsRasell de LunaОценок пока нет
- Report Risk Management For HospitalsДокумент10 страницReport Risk Management For Hospitalsresh0401404100% (1)
- Clinical PortraitДокумент6 страницClinical PortraitDann Francis SarnilloОценок пока нет
- A. Cultural Factors/ethnicity Such As Regard To Elders, Perception of HealthДокумент6 страницA. Cultural Factors/ethnicity Such As Regard To Elders, Perception of Healthlouie john abilaОценок пока нет
- TelemedicineДокумент39 страницTelemedicineraju raj100% (1)
- สอบเข้าม 1วิชาภาษาอังกฤษДокумент25 страницสอบเข้าม 1วิชาภาษาอังกฤษLiwiny Siriporn90% (10)
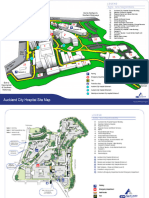
- ACH Site MapTWTДокумент2 страницыACH Site MapTWTyashacnzОценок пока нет
- Unethical Practices in HospitalsДокумент15 страницUnethical Practices in HospitalsSalman SalluОценок пока нет
- Christmas in PragueДокумент2 страницыChristmas in PragueWestEnglishInstituteОценок пока нет
- Mosby's Manual of Diagnostic and Laboratory Tests: Annals of Clinical Biochemistry July 2012Документ3 страницыMosby's Manual of Diagnostic and Laboratory Tests: Annals of Clinical Biochemistry July 2012mustafa aliОценок пока нет
- Courier: Board Makes Final Offer To SEAДокумент12 страницCourier: Board Makes Final Offer To SEAAnonymous 9eadjPSJNgОценок пока нет
- Pubmed - Australia - Conventional - HistoДокумент234 страницыPubmed - Australia - Conventional - HistoHNОценок пока нет
- RENR Review Utech 8Документ34 страницыRENR Review Utech 8natalieshirley100% (3)
- Doctors LahoreДокумент12 страницDoctors LahoreSaima Anwar100% (1)
- ACKS SinisterStoneOfSakkaraДокумент80 страницACKS SinisterStoneOfSakkarasullivbt100% (6)
- NIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewДокумент20 страницNIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewAlexandra PaunОценок пока нет
- Competency 1 Field Finished With 6.2 Saved As PDFДокумент24 страницыCompetency 1 Field Finished With 6.2 Saved As PDFAllisonОценок пока нет
- Planning An Operation Theatre ComplexДокумент4 страницыPlanning An Operation Theatre ComplexRaviraj PisheОценок пока нет
- Role of Amo in Pre Hospital Care andДокумент20 страницRole of Amo in Pre Hospital Care andWan AmeeramirulzamanОценок пока нет
- Patient Care TechnicianДокумент2 страницыPatient Care Technicianapi-78186822Оценок пока нет
- The History of Abnormal PsychologyДокумент57 страницThe History of Abnormal PsychologyMichael B. SilvaОценок пока нет
- 2005step3 IntroductionДокумент91 страница2005step3 Introductioncalven82100% (1)
- List of Doctors and Hospitals in Rheinland-PfalzДокумент6 страницList of Doctors and Hospitals in Rheinland-PfalzNamerah AliОценок пока нет
- Nursing Informatics: Instructor: Ms. Cherry B. BoctotoДокумент68 страницNursing Informatics: Instructor: Ms. Cherry B. BoctotoRegibel Torres100% (1)
- Clinical Science Questions and Answers - Standards MaintainedДокумент7 страницClinical Science Questions and Answers - Standards MaintainedManish JainОценок пока нет
- Clinical Nursing JudgementДокумент6 страницClinical Nursing Judgementapi-353709602Оценок пока нет
- Bahasa Inggris IIIДокумент3 страницыBahasa Inggris IIIAfifah TyasОценок пока нет
- Asepsis and Infection Control Nursing SchoolДокумент20 страницAsepsis and Infection Control Nursing Schoolleonardo orozco100% (1)
- Laporan KPI NICU 2Документ62 страницыLaporan KPI NICU 2fatimahОценок пока нет
- OPDs POF HospitalДокумент2 страницыOPDs POF HospitalIftikhar Hussain Changazi100% (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)