Вам также может понравиться
- Essential Mechanisms in Neurological Pediatric RehabilitationОт EverandEssential Mechanisms in Neurological Pediatric RehabilitationОценок пока нет
- Bayley-III Clinical Use and InterpretationОт EverandBayley-III Clinical Use and InterpretationРейтинг: 2 из 5 звезд2/5 (1)
- M-FUN Assessment ReviewДокумент4 страницыM-FUN Assessment ReviewKishan RamtohulОценок пока нет
- Alberta Infant Motor Scale (AIMS)Документ5 страницAlberta Infant Motor Scale (AIMS)Aditi Desai50% (10)
- Clinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Документ16 страницClinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Jhon Liev100% (2)
- Pediatric Evaluation of Disability Inventory SUMMARYДокумент4 страницыPediatric Evaluation of Disability Inventory SUMMARYFaye ValensoyОценок пока нет
- Alberta Infant ScaleДокумент17 страницAlberta Infant ScaleDuong HungОценок пока нет
- GMFMscoresheetДокумент6 страницGMFMscoresheetAbdur RasyidОценок пока нет
- The Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory SensДокумент8 страницThe Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory Sensapi-238703581Оценок пока нет
- Early, Accurate Diagnosis and Early Intervention in Cerebral PalsyДокумент11 страницEarly, Accurate Diagnosis and Early Intervention in Cerebral PalsyRoberto López MataОценок пока нет
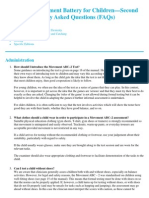
- Movement ABC 2 Frequently Asked QuestionsДокумент8 страницMovement ABC 2 Frequently Asked QuestionsCat Graverobber Iskariot0% (1)
- Alberta Infant Motor Scale Records PDFДокумент6 страницAlberta Infant Motor Scale Records PDFmisobebe80% (5)
- An Integrated Approach - in Every SenseДокумент4 страницыAn Integrated Approach - in Every SenseSpeech & Language Therapy in PracticeОценок пока нет
- Sensory Diet DocumentsДокумент7 страницSensory Diet Documentspratibhaumrariya100% (1)
- Sensorimotor History Questionnaire For Parents of PreschoolДокумент77 страницSensorimotor History Questionnaire For Parents of Preschoolscribdmuthu100% (2)
- Space Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsДокумент4 страницыSpace Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDaNelle McPhaddenОценок пока нет
- Alberta Infant Motor Scale RecordsДокумент6 страницAlberta Infant Motor Scale Recordsgrouch12153% (19)
- Sensory Integration and Praxis Test (SIPT)Документ3 страницыSensory Integration and Praxis Test (SIPT)Sandra Szasz75% (4)
- Occupational Therapy Ia Sample ReportsДокумент11 страницOccupational Therapy Ia Sample Reportssneha duttaОценок пока нет
- Sensory Integration HandoutsДокумент15 страницSensory Integration HandoutsNAA NYC Metro Chapter86% (7)
- Motor DevelopmentДокумент38 страницMotor DevelopmentJesus SanabriaОценок пока нет
- SIPTДокумент2 страницыSIPTAthila Mohamed100% (1)
- IntroClin - Revised Brigance Diagnostic Inventory of Early DevelopmentДокумент22 страницыIntroClin - Revised Brigance Diagnostic Inventory of Early DevelopmentAnnbe Barte100% (4)
- Visual Motor Integration WebinarДокумент5 страницVisual Motor Integration WebinarAnonymous QqyLDoW1100% (1)
- Evaluation and Intervention PlanningДокумент13 страницEvaluation and Intervention PlanningAnup Pednekar100% (1)
- Ot Assessment Template - SelpaДокумент5 страницOt Assessment Template - Selpaapi-417867603100% (1)
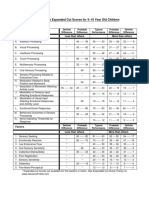
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenДокумент1 страницаSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliОценок пока нет
- Sensory Profile Sample ReportДокумент22 страницыSensory Profile Sample ReportCarolina Recio100% (2)
- Assessments and Outcome Measures of Cerebral PalsyДокумент27 страницAssessments and Outcome Measures of Cerebral Palsyرمزي سويسيОценок пока нет
- Pediatric Evaluation ReportДокумент3 страницыPediatric Evaluation Reportapi-469965619Оценок пока нет
- Sensory DietДокумент11 страницSensory Dietbarbarasanjose100% (7)
- Marcus Evaluation - StruthersДокумент8 страницMarcus Evaluation - Struthersapi-355500890Оценок пока нет
- SI Theory and PracticeДокумент57 страницSI Theory and PracticeMaria Laura Soria100% (1)
- Sensory Profile PowerpointДокумент21 страницаSensory Profile PowerpointFedora Margarita Santander CeronОценок пока нет
- The Movement Assessment of Infants (MAI)Документ52 страницыThe Movement Assessment of Infants (MAI)jalimee86% (7)
- Ot Guidelines Child SpecificДокумент34 страницыOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Occupational Therapy in Neonatal Services and Early Intervention PDFДокумент152 страницыOccupational Therapy in Neonatal Services and Early Intervention PDFLauren100% (1)
- Pediatric Wheelchair Toolkit FINALДокумент6 страницPediatric Wheelchair Toolkit FINALIndiana Family to FamilyОценок пока нет
- Motor Skills Acquisition in The First YearДокумент1 страницаMotor Skills Acquisition in The First YearDaniela Lucena25% (8)
- Bayley Scales of Infant Development IIДокумент2 страницыBayley Scales of Infant Development IIbutterflybaby04Оценок пока нет
- Sensory Profile PowerpointДокумент10 страницSensory Profile PowerpointFedora Margarita Santander CeronОценок пока нет
- Sensory Integration: A Practical Look at The Theory and Model For Intervention by Megan Carrick, MOTR/LДокумент6 страницSensory Integration: A Practical Look at The Theory and Model For Intervention by Megan Carrick, MOTR/LautismoneОценок пока нет
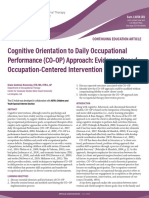
- CO-OP PediatriaДокумент17 страницCO-OP PediatriaCarol Alvarado100% (2)
- Ota Watertown Si Clinical Assessment WorksheetДокумент4 страницыOta Watertown Si Clinical Assessment WorksheetPaulinaОценок пока нет
- Bayley ScalesДокумент7 страницBayley Scalesmrabhilekh100% (1)
- OT Practice August 6 IssueДокумент19 страницOT Practice August 6 IssueThe American Occupational Therapy AssociationОценок пока нет
- AOTA Statement On Role of OT in NICUДокумент9 страницAOTA Statement On Role of OT in NICUMapi RuizОценок пока нет
- Alberta Infant Motor Scale Records PDFДокумент6 страницAlberta Infant Motor Scale Records PDFGUSTAVOОценок пока нет
- CO OP AOTA - July - 2020Документ10 страницCO OP AOTA - July - 2020Ana Claudia GomesОценок пока нет
- Pediatric Assessment&screening ToolsДокумент7 страницPediatric Assessment&screening Toolsdariand100% (1)
- Classic Reflex Hierarchy and ReflexesДокумент8 страницClassic Reflex Hierarchy and ReflexesJaclyn ArpinОценок пока нет
- Sensory Integration in The Home: An OverviewДокумент28 страницSensory Integration in The Home: An OverviewEileen Grant100% (6)
- Using Sensory Integration andДокумент9 страницUsing Sensory Integration andVero MoldovanОценок пока нет
- Feeding and Nutrition in Children with Neurodevelopmental DisabilitiesОт EverandFeeding and Nutrition in Children with Neurodevelopmental DisabilitiesРейтинг: 5 из 5 звезд5/5 (1)
- CERTIFICATION EXAMINATION FOR OCCUPATIONAL THERAPY ASSISTANT (OTA): Passbooks Study GuideОт EverandCERTIFICATION EXAMINATION FOR OCCUPATIONAL THERAPY ASSISTANT (OTA): Passbooks Study GuideОценок пока нет
- Reversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)От EverandReversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)Оценок пока нет
- The Neurological Examination of the Child with Minor Neurological DysfunctionОт EverandThe Neurological Examination of the Child with Minor Neurological DysfunctionОценок пока нет
- Assessing Neuromotor Readiness for Learning: The INPP Developmental Screening Test and School Intervention ProgrammeОт EverandAssessing Neuromotor Readiness for Learning: The INPP Developmental Screening Test and School Intervention ProgrammeРейтинг: 5 из 5 звезд5/5 (1)
- Binocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/AОт EverandBinocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/AОценок пока нет
- ADSMPhase ICFPДокумент12 страницADSMPhase ICFPCamila AlmeidaОценок пока нет
- 7 AIMS Principles Checklist FinalДокумент2 страницы7 AIMS Principles Checklist FinalCamila AlmeidaОценок пока нет
- The Evidence For Integrated Care Healthcare Practice 2015Документ24 страницыThe Evidence For Integrated Care Healthcare Practice 2015Camila AlmeidaОценок пока нет
- Clinical Reasoning in The Health Professions 2008Документ519 страницClinical Reasoning in The Health Professions 2008Mente Sesentayuno100% (1)
- 3 CAHPS HP40 Reporting Measures 2008Документ9 страниц3 CAHPS HP40 Reporting Measures 2008Camila AlmeidaОценок пока нет
- An Integrative Review of Case ManagementДокумент14 страницAn Integrative Review of Case ManagementCamila AlmeidaОценок пока нет
- Lorin W. Anderson, David R. Krathwohl-A Taxonomy For Learning Teaching and Assessing - A Revision of Bloom's Taxonomy of Educational Objetives-Longman (2001)Документ168 страницLorin W. Anderson, David R. Krathwohl-A Taxonomy For Learning Teaching and Assessing - A Revision of Bloom's Taxonomy of Educational Objetives-Longman (2001)Samo Ja100% (5)
- The Lexicon For Behavioral Health and Primary Care Integration USA 2013Документ57 страницThe Lexicon For Behavioral Health and Primary Care Integration USA 2013Camila AlmeidaОценок пока нет
- Disavoia A 2010A PDFДокумент1 страницаDisavoia A 2010A PDFCamila AlmeidaОценок пока нет
- Disavoia A 2010B PDFДокумент1 страницаDisavoia A 2010B PDFCamila AlmeidaОценок пока нет
- Clinical Effectiveness of Care Managers in PDFДокумент10 страницClinical Effectiveness of Care Managers in PDFCamila AlmeidaОценок пока нет
- Disavoia A 2010C PDFДокумент1 страницаDisavoia A 2010C PDFCamila AlmeidaОценок пока нет
- 1438G/A Promoter Polymorphism of The 5-HT2A Gene 1438A Variant Allele of The 5-HTДокумент2 страницы1438G/A Promoter Polymorphism of The 5-HT2A Gene 1438A Variant Allele of The 5-HTCamila AlmeidaОценок пока нет
- Disavoia A 2010C PDFДокумент1 страницаDisavoia A 2010C PDFCamila AlmeidaОценок пока нет
- Management of Comorbid Mental and Somatic PDFДокумент15 страницManagement of Comorbid Mental and Somatic PDFCamila AlmeidaОценок пока нет
- Disavoia A 2010A PDFДокумент1 страницаDisavoia A 2010A PDFCamila AlmeidaОценок пока нет
- Internal Consistency of The INTERMED in Patients With Somatic DiseasesДокумент3 страницыInternal Consistency of The INTERMED in Patients With Somatic DiseasesCamila AlmeidaОценок пока нет
- DeJonge P 2003Документ6 страницDeJonge P 2003Camila AlmeidaОценок пока нет
- Characteristics of Case Management in Primary Care PDFДокумент11 страницCharacteristics of Case Management in Primary Care PDFCamila AlmeidaОценок пока нет
- Disavoia A 2010B PDFДокумент1 страницаDisavoia A 2010B PDFCamila AlmeidaОценок пока нет
- The Biopsychosocial Model ... 2017Документ10 страницThe Biopsychosocial Model ... 2017Camila AlmeidaОценок пока нет
- Clinical Effectiveness of Care Managers in PDFДокумент10 страницClinical Effectiveness of Care Managers in PDFCamila AlmeidaОценок пока нет
- Systematic Review of Integrated Models of Health Care Delivered PDFДокумент18 страницSystematic Review of Integrated Models of Health Care Delivered PDFCamila AlmeidaОценок пока нет
- A Pilot Study of A Community Health Agent-Led Type 2 Diabetes Self-Management Program Using Motivational Interviewing-Based Approaches in A Public Primary Care Center in São Paulo BrazilДокумент10 страницA Pilot Study of A Community Health Agent-Led Type 2 Diabetes Self-Management Program Using Motivational Interviewing-Based Approaches in A Public Primary Care Center in São Paulo BrazilCamila AlmeidaОценок пока нет
- A Pilot Study of A Community Health Agent-Led Type 2 Diabetes Self-Management Program Using Motivational Interviewing-Based Approaches in A Public Primary Care Center in São Paulo BrazilДокумент10 страницA Pilot Study of A Community Health Agent-Led Type 2 Diabetes Self-Management Program Using Motivational Interviewing-Based Approaches in A Public Primary Care Center in São Paulo BrazilCamila AlmeidaОценок пока нет
- 1748 5908 4 50 PDFДокумент15 страниц1748 5908 4 50 PDFCamila AlmeidaОценок пока нет
- Co - and Multimorbidity Patterns in Primary Care Based On Episodes PDFДокумент8 страницCo - and Multimorbidity Patterns in Primary Care Based On Episodes PDFCamila AlmeidaОценок пока нет
- Challenges To Primary Care From Co and MultimorbidityДокумент2 страницыChallenges To Primary Care From Co and MultimorbidityCamila AlmeidaОценок пока нет
- INTERMED Elderly Self Assessment English Version 1.0.0Документ4 страницыINTERMED Elderly Self Assessment English Version 1.0.0Camila AlmeidaОценок пока нет
- DSSSB PRT Vacancy 2019Документ8 страницDSSSB PRT Vacancy 2019MONTYОценок пока нет
- Candidate'S Guide For The Cttic Standard Certification Examination in TranslationДокумент5 страницCandidate'S Guide For The Cttic Standard Certification Examination in Translationa7khalidОценок пока нет
- Alliance Manchester Business SchoolДокумент14 страницAlliance Manchester Business SchoolMunkbileg MunkhtsengelОценок пока нет
- Argumentation and Debate Course SyllabusДокумент4 страницыArgumentation and Debate Course SyllabusFernand CJ CastroОценок пока нет
- Additional Maths SBA FINALДокумент36 страницAdditional Maths SBA FINALJaniah Aaliyah M. Drakes42% (24)
- The Scientific Method and Components of A Controlled Experiment PDFДокумент36 страницThe Scientific Method and Components of A Controlled Experiment PDFJanen MacanasОценок пока нет
- TOEFL ITP Practice TestsДокумент2 страницыTOEFL ITP Practice TestsArlen Sasmita0% (1)
- VedantuДокумент74 страницыVedantuHarshit RoyОценок пока нет
- Cause and Effect EssayДокумент6 страницCause and Effect EssayNurIzzatiОценок пока нет
- Wii SVBH PDFДокумент3 страницыWii SVBH PDFJaspal SinghОценок пока нет
- Hallinger Murphy (1985) PIMRSДокумент32 страницыHallinger Murphy (1985) PIMRSzamri abdullahОценок пока нет
- Presented By: Mubashir Hassan Prekshya Panth Priyanka Rajbhandari Neelam Kr. Patel Neeraj SinghalДокумент19 страницPresented By: Mubashir Hassan Prekshya Panth Priyanka Rajbhandari Neelam Kr. Patel Neeraj SinghalANURADHA CHHIPAОценок пока нет
- IELTS Reading Strategies Summarized PDFДокумент3 страницыIELTS Reading Strategies Summarized PDFDinaj AttanayakaОценок пока нет
- Masters Thesis Marking SheetДокумент4 страницыMasters Thesis Marking Sheetnitinsharma.gkvОценок пока нет
- ENM401E 20aa15 TL203 2 BДокумент4 страницыENM401E 20aa15 TL203 2 BHadrien FaryalaОценок пока нет
- Recruitment of Clerical Staff in Oriental Bank of Commerce: Registration #: Full Name: Akhil AroraДокумент2 страницыRecruitment of Clerical Staff in Oriental Bank of Commerce: Registration #: Full Name: Akhil AroraAkhil AroraОценок пока нет
- Engl 393 Minor Homework 1Документ3 страницыEngl 393 Minor Homework 1api-460966246Оценок пока нет
- Practicum Observation LogДокумент1 страницаPracticum Observation Logapi-343608586Оценок пока нет
- Correct Grammar UsageДокумент63 страницыCorrect Grammar UsageChristopher PjunatasОценок пока нет
- Culminating-Activity Shs Humss q1 Specialized As-Of-Oct6-2Документ40 страницCulminating-Activity Shs Humss q1 Specialized As-Of-Oct6-2Nhormie Maan Salazar100% (2)
- PMI SP HandbookДокумент57 страницPMI SP HandbookMohamed Aladdin100% (1)
- Identification (ID) RequirementsДокумент2 страницыIdentification (ID) RequirementsNandu RapakaОценок пока нет
- Draft Guidelines For Online RevalidaДокумент2 страницыDraft Guidelines For Online RevalidaCamille GrandeОценок пока нет
- George Morris: Mechanical Engineer Having Rich Experience of Above 3years in Oil and Gas Construction ObjectiveДокумент6 страницGeorge Morris: Mechanical Engineer Having Rich Experience of Above 3years in Oil and Gas Construction Objectivedavidgeorge143Оценок пока нет
- Field Study 1 Ep 8 Close Encounter With The School Curriculum Fabrero Jayrel RДокумент6 страницField Study 1 Ep 8 Close Encounter With The School Curriculum Fabrero Jayrel RJayrel FabreroОценок пока нет
- Supplemental English High School Grade 7 2nd Q 2Документ8 страницSupplemental English High School Grade 7 2nd Q 2maria ceryll100% (1)
- IELTS Speaking Sample QuestionsДокумент969 страницIELTS Speaking Sample Questionsmay mon0% (1)
- Experimental Research (Scientific Inquiry) : Mcgraw-HillДокумент38 страницExperimental Research (Scientific Inquiry) : Mcgraw-HillRabia Tabassum DhanotarОценок пока нет
- CPA Australia-Stategic Management Accounting-2ND-EDN (2019)Документ740 страницCPA Australia-Stategic Management Accounting-2ND-EDN (2019)Trinh Pham100% (8)
- Year 11 Mock Examination InformationДокумент15 страницYear 11 Mock Examination InformationChrist's SchoolОценок пока нет