Академический Документы
Профессиональный Документы
Культура Документы
The Economic Burden of Dementia in China, 1990-2030: Implications For Health Policy
Загружено:
Eny A. WatumlawarОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
The Economic Burden of Dementia in China, 1990-2030: Implications For Health Policy
Загружено:
Eny A. WatumlawarАвторское право:
Доступные форматы
Research
The economic burden of dementia in China, 19902030: implications
for health policy
JunfangXu,a JianWang,b AndersWimo,c LauraFratiglionid & ChengxuanQiud
Objective To quantify and predict the economic burden of dementia in China for the periods 19902010 and 20202030, respectively, and
discuss the potential implications for national public health policy.
Methods Using a societal, prevalence-based, gross cost-of-illness approach and data from multiple sources, we estimated or predicted
total annual economic costs of dementia in China. We included direct medical costs in outpatient and inpatient settings, direct non-medical
costs e.g. the costs of transportation and indirect costs due to loss of productivity. We excluded comorbidity-related costs.
Findings The estimated total annual costs of dementia in China increased from 0.9 billion United States dollars (US$) in 1990 to US$47.2billion
in 2010 and were predicted to reach US$69.0billion in 2020 and US$114.2billion in 2030. The costs of informal care accounted for 94.4%,
92.9% and 81.3% of the total estimated costs in 1990, 2000 and 2010, respectively. In China, population ageing and the increasing prevalence
of dementia were the main drivers for the increasing predicted costs of dementia between 2010 and 2020, and population ageing was the
major factor contributing to the growth of dementia costs between 2020 and 2030.
Conclusion In China, demographic and epidemiological transitions have driven the growth observed in the economic costs of dementia
since the 1990s. If the future costs of dementia are to be reduced, China needs a nationwide dementia action plan to develop an integrated
health and social care system and to promote primary and secondary prevention.
Introduction Methods
According to the 2013 Alzheimers Disease International In this cost-of-illness study, we used a prevalence-based, bot-
report, about 44.4million people were living with de- tom-up approach to quantify or predict the costs of dementia
mentia in 2013 and this number is expected to reach an in China between 1990 and 2030, from a societal perspective.
estimated 75.6 million by 2030. 1 In China, which has the We categorized all the costs into three classes:12,13 (i)direct
largest population of people with dementia, the prevalence medical costs, that is goods and service costs related to the
of dementia appears to have increased steadily between diagnosis and treatment of inpatients and outpatients with
1990 and 2010. 2,3 However, this trend might be partly dementia; (ii)direct non-medical costs, that is transport costs
attributed to temporal variations in the methods used to and costs related to formal care in nursing homes or informal
estimate such prevalence.4 The results of a national survey care at home; and (iii)indirect costs resulting from dementia-
in 20082009 indicated that dementia was more common attributable loss of productivity.
in rural areas than in urban settings. 5 Given the rapid
Data sources
growth of the elderly population in China, 6 dementia is
expected to pose tremendous challenges to the national We used multiple data sources for all estimates. We used
health-care system and to the sustainable development of age-specific prevalence of dementia in China, for the period
the national economy. 19902010, derived from a comprehensive systematic review.3
Most cost-of-illness studies for dementia have been car- From the electronic health records of the facilities, we collected
ried out in high-income countries such as Sweden, the United cost data for patients with diagnosed dementia who were ad-
Kingdom of Great Britain and Northern Ireland and the United mitted either to the Shandong Centre for Mental Health the
States of America.711 The economic costs of dementia in China only provincial psychiatric hospital in the eastern province
which have yet to be investigated in detail are likely to dif- of Shandong between 1 January 2005 and 31 March 2014
fer, both in magnitude and type, from those in such distant or to the Daizhuang Psychiatric Hospital one of the oldest
high-income countries. psychiatric hospitals in China and also in Shandong prov-
In this study, we sought to estimate and predict the costs of ince between 1 January 2012 and 30 September 2014. The
dementia in China for the periods 19902010 and 20202030, routine electronic health records include sociodemographic
respectively. It was hoped that, by quantifying the economic data and data on clinical diagnosis and disease classification,
costs of dementia, Chinese policy-makers would be motivated itemized costs, e.g. for drugs, examinations and beds. In
to develop a nationwide action plan, prioritize policies on each of the two study facilities, dementia was diagnosed and
dementia-related care and research and reduce the economic defined according to the International statistical classification
and societal burdens of dementia in China. of diseases and related health problems, 10th revision.14 We
a
Research Centre for Public Health, Tsinghua University, Beijing, China.
b
Centre for Health Economic Experiments and Public Policy, Shandong University, Jinan, China.
c
Division of Neurogeriatrics, Karolinska Institutet, Stockholm, Sweden.
d
Ageing Research Centre, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm University, Gvlegatan 16, 113 30 Stockholm,
Sweden.
Correspondence to Chengxuan Qiu (email: chengxuan.qiu@ki.se).
(Submitted: 3 December 2015 Revised version received: 2 September 2016 Accepted: 16 September 2016 Published online: 18 October 2016)
18 Bull World Health Organ 2017;95:1826 | doi: http://dx.doi.org/10.2471/BLT.15.167726
Research
Junfang Xu et al. Economic burden of dementia in China
Table 1. Estimated numbers of people Table 2. Predicted age-specific prevalence of dementia and numbers of people with
with dementia, China, 1990, dementia, China, 2020 and 2030
2000 and 2010
Age in years 2020 2030
Variable Thousands of people with
Prevalence Thousands of cases Prevalence Thousands of cases
dementiaa
(%) (%)
1990 2000 2010 6064 1.5 1121.1 1.7 1879.0
n=2479.7 n=5148.4 n=9615.6
6569 3.0 2117.3 3.4 2966.8
Age in 7074 5.3 2340.7 6.0 3661.7
years 7579 9.7 2593.2 11.0 5477.5
6064 314.3 454.6 792.0 8084 16.6 2717.8 18.8 4547.9
6569 462.0 726.9 1060.7 8589 27.8 2096.8 31.5 2997.0
7074 654.7 989.7 1569.5 90 47.4 1082.1 53.9 1760.8
7579 726.1 1099.1 2027.4 60a 5.8 14069.0 6.7 23290.7
8084 655.0 948.3 1956.5
The values shown cover all of the expected dementia cases aged at least 60years.
a
8589 435.7 598.3 1369.7
90 231.9 331.6 839.7
Sex Table 3. Estimated costs of dementia, China, 1990, 2000 and 2010
Male 1313.1 1942.8 3628.5
Cost item Year
Female 2166.6 3205.6 5987.1
Residence 1990 2000 2010
Urban 2109.8 3121.5 5829.9 Costs per case (US$)
Rural 1370.0 2026.9 3785.7 Direct medical costs
NOTE: Inconsistencies arise in some values due Hospitalization cost 37.1 370.0 1004.0
to rounding. Outpatient care cost 0.5 5.0 148.8
a
Estimates based on a systematic review of the
prevalence of dementia in China.3 Direct non-medical costs
Nursing home care 47.4 222.4 4468.1
Transportation 0.5 4.9 143.8
excluded 26 patients with dementia who
Informal care 271.5 1184.0 4635.4
were diagnosed as having other chronic
Indirect costs
conditions that needed treatment, e.g.
anxiety, diabetes or hypertension, leav- Cost due to DALYs lost 4.8 22.9 87.6
ing data from the records of 146 patients Total for cases living at home 314.4 1586.8 6019.6
with dementia in our analysis. We also Total for cases living in nursing homes 90.3 625.2 5852.3
searched the China National Knowledge National costs (US$ millions)
Infrastructure, PubMed and Wanfang Direct medical costs
bibliographic databases for studies, on Hospitalization cost 6.3 93.3 473.0
the use of health resource by people Outpatient care cost 1.8 26.1 1431.0
with dementia in China, published be- Direct non-medical costs
tween 1 January 1990 and 31 July 2015. Nursing home care 23.1 160.3 6014.9
The search terms included Alzheimers Transportation 0.1 1.2 67.8
disease, China, cost burden, demen- Informal care 812.4 5242.3 38332.0
tia, economic burden, formal care Indirect costs
and informal care. We obtained costs
Cost due to DALYs lost 16.7 118.1 842.3
for outpatient visits and transporta-
Total for all cases 860.4 5641.4 47161.0
tion from a published study.15 Data on
Sex of case
demographics and wages came from
the China Statistical Yearbook 2015.16 Men 324.7 2128.6 17796.5
The United Nations population projec- Women 535.7 3512.2 29364.2
tions for China17 and predictions of the Residence of case
prevalence of dementia based on data Urban 514.6 3375.0 28578.9
from a systematic review3 were used to Rural 345.8 2266.4 18582.1
estimate the total numbers of people DALYs: disability-adjusted life-years; US$: United States dollars.
in China who would have dementia in Note: All the estimated costs were converted to United States dollar (US$) values in January 2015, when
2020 and 2030. US$1 was equivalent to about 6.2 Chinese yuan.
Cost estimates
care and transportation. Our estimates bed care, were based on the mean values
For our estimates we included costs for of hospitalization costs, which included of the costs recorded in the electronic
hospitalization, formal care, informal the costs of all medicines, clinical ex- health records of the two study facili-
care, loss of productivity, outpatient aminations, specialist consultations and ties and the values given in a published
Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726 19
Research
Economic burden of dementia in China Junfang Xu et al.
article15 all weighted according to the to estimate the relative contributions patients instead of 4.9% would seek
sample sizes. Our estimates of the costs made by the ageing population and professional care.21
of formal care were similarly weight- changes in the age-specific prevalence
ed mean values based on published of dementia to the predicted future costs
data.18,19 Informal care costs were esti- of dementia.26 When the relevant data
Results
mated assuming that a carer, who might on medical costs for particular years The total number of people with demen-
otherwise be earning the national mean were missing, we assumed that those tia in China was estimated to be about
salary,13 spent a mean of 6.3hours per costs would have increased by the same 3.5 million in 1990, 5.1 million in 2000
day20 giving care to each dementia case amount as the per-capita gross domestic and 9.6 million in 2010 (Table1). The
in informal care at home. We assumed product (GDP). overall prevalence of dementia among
that, during the observational periods, We conducted multiple sensitivity people aged at least60years was pro-
86% of Chinese dementia cases were re- analyses to assess the impact of varia- jected to increase from 5.8% in 2020 to
ceiving informal care at home and that tions in the key input parameters on 6.7% in 2030 (Table2). The total number
4.9% of such cases would seek formal our primary estimates. Specifically, we of people with dementia in China was
care.13,21 We estimated the numbers of estimated the total costs of dementia projected to reach 14.1 million by 2020
disability-adjusted life-years (DALYs) by (i)using prevalence data derived and 23.3 million by 2030.
lost because of dementia using each from a different systematic review2 that Between 1990 and 2010, the mean
cases dementia severity score, as- yielded more conservative estimates of annual costs of formal and informal care
sessed using the Global Deterioration the prevalence of dementia than those for each dementia case increased more
Scale,22 and different weights for each that we used3 for our primary estimates; than60-fold and more than 18-fold,
of seven levels of severity.23 Costs of the (ii)assuming that medical costs would respectively (Table3). Over the same
productivity lost because of dementia- increase 5% every year; (iii)using the period, the national total annual costs of
related disability were then estimated. minimum and maximum values in- dementia increased more than 50-fold,
For these estimations, we assumed that stead of the overall mean for the hours from about US$0.9billion in 1990 to
each person aged at least 60years had spent on informal care;27 (iv)using the approximately US$47.2billion, or about
a mean productivity weight of 0.1 and means of the minimum and maximum 0.7% of Chinas GDP in 2010.
we used an annual discount rate of 3.5% values recorded, in Chinas 22 prov- The total costs of dementia were
to adjust the costs to 2015 values. 24 inces, five autonomous regions and four projected to reach US$69.0billion in
Outpatient care costs included the costs municipalities, for an informal carers 2020 and US$114.2 billion in 2030
of treatments and specialist consulta- wages instead of the overall national (Fig.1). The ageing population and in-
tions received in clinics or at home.15 mean value; (v)assuming that dementia creases in dementia prevalence appeared
Transportation costs comprised the cases aged at least 60years had a mean to be the major driving factors for the
costs travelling to and from medical productivity weight of 0.5027 instead high costs of dementia in 20102020
centres.15 of 0.1; (vi)assuming that 70% or 99% and the ageing population also appeared
All the estimated costs were con- of people with dementia instead of to be the dominant force behind the
verted to United States dollar (US$) 86% would live at home;7 and (vii)as- growth of dementia costs between 2020
values in January 2015, when US$1 was suming that 60.4% or 0.4% of dementia and 2030 (Fig.2).
equivalent to about 6.2 Chinese yuan.
Statistical analysis
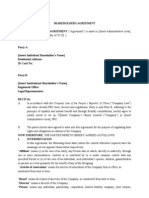
Fig. 1. Estimated total annual costs of dementia, China, 19902030
We estimated the numbers of people
with dementia in China in 1990, 2000
and 2010 by multiplying the age-specific 120
114.2
prevalence of dementia 3 by the cor-
responding numbers of people in each 100
age group in the population. For our
predictions for 2020 and 2030, we used
Total cost (US$ billions)
80
age-specific prevalence derived using a
69.0
regression model and the relevant data
from a comprehensive review.3 We esti- 60
mated the total annual costs of demen- 47.2
tia by multiplying the mean costs per 40
patient by the total number of patients
with dementia. Total annual costs for
20
2020 and 2030 were projected using a 5.6
dynamic general disequilibrium model25 0.9
and assuming that the use of health 0
1990 2000 2010 2020 2030
resources by a dementia case was con-
Year
stant while the elderly population grew
and the age-specific prevalence of de-
US$: United States dollars.
mentia varied over time. We employed Note: All the estimated costs were converted to United States dollar (US$) values in January 2015 when
the Laspeyres decomposition method US$1 was equivalent to about 6.2 Chinese yuan.
20 Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726
Research
Junfang Xu et al. Economic burden of dementia in China
According to our estimates, the care of an elderly family member is costs for hospitalization due to dementia
costs of informal care for dementia traditionally perceived as an act of filial indicated that such costs increased more
accounted for 94.4%, the total costs of piety and dementia cases are therefore slowly between 2000 and 2010 than be-
dementia care in China in 1990, decreas- generally kept out of nursing homes.15,33 tween 1990 and 2000. It seems likely that
ing to 92.9% in 2000 and 81.3% in 2010 In rural areas there is also a lack of facili- hospitalization costs became more stable
(Fig.3). In contrast, the costs of formal ties and professional carers for dementia in 2003, when the Chinese government
care accounted for just 2.7% of the total cases.34 There is no consensus on how to launched a programme of health-care
costs in 1990, increasing to 2.8% in estimate the costs of informal care with reform designed to make medical treat-
2000 and 12.8% in 2010. Hospitaliza- regard to care hours, costs per hour or ment more accessible.35 Our data also
tion costs accounted for only about 1% types of caregiver or the potential in- revealed a substantial increase in the
of total costs in each year between 1990 direct costs, e.g. of lost productivity, in- proportion of the total costs of dementia
and 2010. curred by informal caregivers.7,13,20 As in care attributed to formal care between
The results of our sensitivity analy- previous estimates of the global costs of 2000 and 2010. In countries with rapid
ses indicated that variations in informal dementia,7,13 we assumed that informal economic growth, the responsiveness
care hours, prevalence of dementia and caregivers would be earning the national of the quantity demanded for a service
productivity weighting had a substantial mean wage if they were not caring for to a change in the income of the people
impact on estimates of the total costs of dementia cases. Our estimates of the demanding that service, that is, the
dementia, whereas changes in medical
prices, wages and the proportions of
patients living at home or seeking pro-
Fig. 2. Attribution of the causes of the changes in total annual costs of dementia care,
China, 20102030
fessional care had relatively little impact
on such estimates (Table4).
16
Discussion 20102020
14
Increasing costs of dementia
Increase in total costs (US$ billions)
12
In China, from an age of 60years, the
prevalence of dementia almost doubles 10
every five years and, as elsewhere,28,29
about half of those who have survived to 8
an age of at least 90years are affected by
6
dementia. According to our estimates,
the economic burden of dementia in 4
China will increase substantially over
the next few decades and this increase 2
will be driven primarily by population
ageing and the increasing prevalence 0
6064 6569 7074 7579 8084 8589 >90
of dementia. Our estimates of the total
Age (years)
costs of dementia in China for 2010
and 2030 represent about 7.8% of the 16
20202030
estimated US$604billion global cost
14
in 2010 and 10% of the forecasted
Increase in total costs (US$ billions)
US$1110 billion global cost in 2030.1,7 12
Our primary estimates of dementia costs
are probably underestimates as they ig- 10
nore the effects, on the costs of care, of
8
home visits by professional careers, the
predicted increases in the prevalence of 6
diabetes, hypertension and other risk
factors for dementia30 and the predicted 4
increases in the use of medical services
and devices. 2
Our analyses indicated that, in
0
China, informal care accounted for more 6064 6569 7074 7579 8084 8589 >90
than 80% of the total dementia costs in Age (years)
2010. This proportion is consistent with Total change Attributable to dementia prevalence
the global trend revealed by a systematic Attributable to ageing population
review31 but higher than the proportion,
of about 60%, reported for low- and US$: United States dollars.
middle-income countries by the World Note: All the estimated costs were converted to United States dollar (US$) values in January 2015 when
Health Organization. 32 In China, the US$1 was equivalent to about 6.2 Chinese yuan.
Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726 21
Research
Economic burden of dementia in China Junfang Xu et al.
tors for dementia, e.g. cardiovascular
Fig. 3. Relative contributions made by six cost items to the total annual costs of
disease, that can be targeted for primary
dementia care, China, 1990, 2000 and 2010
prevention.41 Current intervention strat-
egies against cardiovascular disease are
100 likely to be effective in delaying demen-
2.7 2.8
tia onset. The declining incidence of de-
12.8
90
mentia in some high-income countries
may be attributable to improvements in
the control of other risk factors such as
80 diabetes, hypertension and smoking.4245
94.4 92.9 81.3 In addition, in settings where effective
medical and social-care interventions
70 are available, screening for the early de-
tection of dementia may be costeffec-
Proportion of total costs (%)
60
tive.46,47 Geriatricians in clinical settings
should be alert to the first symptoms and
signs of the dementia syndrome. Early
50 interventions for dementia may delay
entry into nursing homes and reduce
the overall costs of care.48
40
Strengths and limitations
Our estimates were based on data from
30
multiple sources. The cost data on the
use of health resources by dementia
20 cases were from itemized routine hos-
pital records, prevalence data were from
a comprehensive systematic review3 and
10 United Nations population projections
and data from the National Bureau of
Statistics of China represented the most
0 authoritative sources for demographic
1990 2000 2010
Year and income data. Our study had several
limitations. First, given the consider-
Hospitalization Outpatient care Transportation Informal care DALYs lost
able variations in economy, cultures,
Nursing home care
health-care systems, social welfare
DALYs: disability-adjusted life-years. and traditions across China, cost data
from two health facilities in Shandong
province are unlikely to be nationally
income elasticity of demand, usually integrated health and social-care sys- representative. We partly addressed this
increases the use of formal care. Given tem, including improvements in the ef- concern by weighting our estimates and
the Chinese tradition of home care and ficiency of dementia care and improved performing multiple sensitivity analyses.
the debate over whether formal care can health education and financial and social The values for income per capita, health
ever meet all of the emotional and psy- support for dementia cases and their expenditure and hospital costs for Shan-
chological needs of dementia cases,36,37 caregivers. Dementia care might be dong province are similar to the mean
it remains to be seen whether increasing integrated with the national programme national values.49 Second, the growth
wealth in China will have much effect on for critical illness insurance. Informal rate of medical prices is generally faster
the uptake of formal care for dementia caregivers could be taught knowledge than that of the GDP values we used to
cases. However, it seems possible that and skills relevant to dementia care.40 fill gaps in the data on dementia costs.
Chinas one-child policy, which was Central or local governments could Given the increasing awareness and use
implemented in the late 1970s and only adopt preferential tax policies or offer of health services for dementia, it also
phased out from 2015, will leave too other financial incentives to encour- seems likely that the costs of medical
few adults in the 2030s to give sustain- age nongovernmental organizations to services will increase more rapidly in
able informal care to all of the dementia participate more in dementia-related the coming decades than by 5% annu-
cases.38,39 care services and education. ally, that is, by the rate we used in our
Policy-makers also need to estab- sensitivity analysis. Third, as people
Implications for health policy
lish a strategic action plan designed to with dementia often suffer from other
In China, public health policy needs promote the primary and secondary chronic health conditions,50,51 comor-
to be tailored to address the economic prevention of dementia. In the past few bidities might reduce the accuracy of
burden posed by dementia. There needs decades, epidemiological studies have our estimates of dementia costs. Fourth,
to be greater focus on developing an identified several modifiable risk fac- data on the proportion of patients with
22 Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726
Research
Junfang Xu et al. Economic burden of dementia in China
Table 4. Changes in the estimated annual costs of dementia according to variations in the key parameters considered in sensitivity
analyses, China, 1990, 2000, 2010, 2020 and 2030
Parameter varied Changes in estimated total costs,a US$ billions (%)
1990 2000 2010 2020 2030
Prevalence of dementia b
0.5 (62.3) 1.6 (27.8) 15.8 (33.5) 25.0 (27.6) 34.6 (23.1)
Medical costs
5% annual increase between 2010 and 2030, ND ND ND +7.3 (+9.6) +31.7 (+21.7)
instead of 0%
Informal care in hours per day
2.5 instead of 6.3 0.5 (56.9) 3.2 (56.0) 23.1 (49.0) 33.8 (49.0) 56.0 (49.0)
8.9 instead of 6.3 +0.3 (+39.0) +2.2 (+38.4) +15.8 (+33.5) +23.1 (+33.5) +38.3 (+33.5)
Wage for caregiversc
Minimum instead of mean ND 1.2 (21.4) 9.3 (19.8) 13.7 (19.8) 22.6 (19.8)
Maximum instead of mean ND +2.1 (+37.6) +5.5 (+11.7) +8.1 (+11.7) +13.4 (+11.7)
Productivity weight for those aged 60
years
0.5 instead of 0.1 +0.2 (+27.2) +1.5 (+27.5) +11.2 (+23.8) +16.4 (+23.8) +27.2 (+23.8)
Percentage of cases living at home
70% instead of 86% 0.1 (14.5) 0.8 (14.0) 0.3 (0.5) 0.4 (0.5) 0.6 (0.5)
99% instead of 86% +0.1 (+11.8) +0.6 (+11.4) +0.2 (+0.4) +0.3 (+0.4) +0.5 (+0.4)
Percentage of cases seeking professional
treatment
60.4% instead of 4.9% +0.1 (+8.5) +1.1 (+19.0) +6.1 (+13.0) +9.0 (+13.0) +14.8 (+13.0)
0.4% instead of 4.9% +0.01 (+0.6) +0.1 (+1.5) +0.5 (+1.1) +0.7 (+1.1) +1.2 (+1.1)
ND: not determined; US$: United States dollars.
a
Compared with the primary estimates of costs.
b
Prevalence values given in one systematic review,2 that is, 1.3% in 1990, 2.9% in 2000 and 3.6% in 2010, instead of the values used for the primary estimates, that is,
4.9% in 1990, 5.4% in 2000 and 7.5% in 2010.3
c
We used the national mean of the minimum per-capita wages recorded in Chinas 22 provinces, five autonomous regions and four municipalities, that is, US$1006.6
in 2000 and US$3872.6 in 2010, or the national mean of the corresponding maximum wages, that is, US$1812.6 in 2000 and US$5774.4 in 2010, instead of the
overall national mean wages of US$1505.3 in 2000 and US$5893.4 in 2010. We predicted the corresponding values for 2020 and 2030 from the values for 2010.
Note: All the estimated costs were converted to United States dollar (US$) values in January 2015, when US$1 was equivalent to about 6.2 Chinese yuan
dementia seeking professional care were Given the huge economic burden of Foundation of Shandong University
very limited. Finally, while we used a dementia, policy-makers in China are in China (project 2012JC038), and the
dynamic model in our projection to advised to make dementia a national Swedish Brain Power network. JX was
account for the ageing population and health priority and to develop a stra- supported by the Sino-Foreign Co-cul-
changes in prevalence of dementia over tegic nationwide action plan. Failure ture Programme of Shandong University
time, alterations in other factors e.g. to take appropriate action now will for her training, as a visiting doctoral stu-
use of medical devices, prevalence of allow the economic burden of demen- dent, at the Karolinska Institutet. CQ re-
risk factors for dementia and the hiring tia to grow even further and could, ceived grants from the Swedish Research
of professional caregivers may have in the long-term, cause dysfunction Council (grant 20152531), the Swedish
reduced the accuracy of our predictions. throughout Chinas entire health-care Research Council for Health, Working
If, in the future, additional data become system. Life and Welfare (grant 20141382) and
available, alternative approaches such as the Karolinska Institutet.
micro-simulation may provide better Acknowledgements
cost estimates.52,53 We thank the staff of the two study Competing interests: AW received grants
In conclusion, demographic and facilities. and personal fees from Eli-Lilly, grants
epidemiological transitions in the past from Nutricia, Ingenix and Envivo and
two decades have driven substantial Funding: This work was supported in personal fees from Lundbeck. AW owns
growth in the economic costs of de- part by grants from the National Natural the copyright on the Resource Use in
mentia in China. This trend is likely Science Foundation of China (project Dementia instrument, for which he re-
to continue over the next two decades. 71373146), the Independent Innovation ceives royalties.
Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726 23
Research
Economic burden of dementia in China Junfang Xu et al.
:20301990
114.2 2020 69.0
%94.4 .2030 2030-2020 2010-1990
1990 %81.3 %92.9 .
. 2010 2000
2010
2020
.
.2030 2020
.
. .
47.2 1990 0.9
. 2010
19902030
1990 2010 1142 1990
2020 2030 2000 2010 94.4
92.9 81.3
2010 2020
2020 2030
1990 9 2010 472
2020 690 2030
Rsum
Charge conomique de la dmence en Chine de1990 2030: consquences sur la politique sanitaire
Objectif Calculer et prvoir la charge conomique de la dmence en atteindra69,0milliards dUS$ en2020 et114,2milliards dUS$ en2030.
Chine pour les priodes stendant de19902010 et de20202030 Le cot des soins informels reprsente94,4%, 92,9% et 81,3% du cot
respectivement, et analyser les consquences potentielles sur la total estim pour les annes1990,2000 et2010, respectivement. En
politique nationale de sant publique. Chine, le vieillissement de la population et la prvalence croissante de
Mthodes laide dune approche socitale relative au cot brut de la la dmence taient les principaux facteurs de laugmentation des cots
maladie fonde sur la prvalence et de donnes provenant de diffrentes lis la dmence prvus entre2010 et2020, et le vieillissement de la
sources, nous avons effectu une estimation et une prvision du cot population tait le principal facteur contribuant laugmentation des
conomique annuel total de la dmence en Chine. Nous avons pris en cots lis la dmence entre2020 et2030.
compte les cots mdicaux directs dans les services de consultation Conclusion En Chine, les transitions dmographiques et
externe et en milieu hospitalier, les cots non mdicaux directs les pidmiologiques ont entran depuis les annes90 une augmentation
cots de transport, par exemple et les cots indirects dus une des cots conomiques lis la dmence. Afin de rduire les futurs cots
perte de productivit. Nous navons pas tenu compte des cots lis lis la dmence, la Chine doit laborer un plan daction dampleur
la comorbidit. nationale lgard de la dmence pour pouvoir mettre en place un
Rsultats Daprs nos estimations, le cot annuel total de la dmence systme de sant et de services sociaux intgr et promouvoir la
en Chine est pass de 0,9milliard de dollars des tats-Unis (US$) prvention primaire et secondaire.
en1990 47,2milliards dUS$ en2010, et nos prvisions indiquent quil
24 Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726
Research
Junfang Xu et al. Economic burden of dementia in China
, 19902030.
1990 47,2 2010;
1990 2010 69 2020
2020 2030, 114,2 2030.
94,4; 92,9 81,3%
. 1990, 2000 2010 .
,
2010 2020
, , ;
,
, , . 2020 2030.
, (, ,
) , , 1990-.
. ,
, .
,
0,9 .
Resumen
La carga econmica de la demencia en China, 19902030: implicaciones para la poltica sanitaria
Objetivo Cuantificar y predecir la carga econmica de la demencia en hasta los 69000millones de USD en 2020 y los 114200millones de
China durante los periodos comprendidos entre 1990 y 2010 y entre USD en 2030. Los costes de la atencin informal sumaban un 94,4%,
2020 y 2030, respectivamente, y analizar las posibles implicaciones para un 92,9% y un 81,3% del total de costes estimados en 1990, 2000 y
la poltica sanitaria pblica del pas. 2010, respectivamente. En China, el envejecimiento demogrfico y la
Mtodos Utilizando un enfoque social, basado en la prevalencia y creciente prevalencia de la demencia fueron los principales impulsores
coste bruto de la enfermedad, as como informacin de varias fuentes, del aumento de los costes de la demencia previstos entre 2010 y 2020,
se estim o se predijo el total de costes econmicos anuales de la y el envejecimiento demogrfico fue el principal factor que contribuy
demencia en China. Se incluyeron los costes mdicos directos en al crecimiento de los costes de la demencia entre 2020 y 2030.
entornos ambulatorios y hospitalarios, los costes no mdicos directos Conclusin En China, las transiciones demogrficas y epidemiolgicas
(por ejemplo, los costes de transporte) y los costes indirectos derivados han impulsado el crecimiento observado en los costes econmicos de la
de la prdida de productividad. No se incluyeron los costes relacionados demencia desde la dcada de los 90. Si el objetivo es reducir los futuros
con la comorbilidad. costes de la demencia, China necesita un plan de accin nacional contra
Resultados El total de costes anuales estimados de la demencia en la demencia para desarrollar un sistema de atencin sanitaria y social
China aument de 900 millones de dlares estadounidenses (USD) en integrado y fomentar la prevencin primaria y secundaria.
1990 a 47200millones de USD en 2010, y se prev que aumentarn
References
1. Policy brief for heads of government: the global impact of dementia 2013- 6. Zhang NJ, Guo M, Zheng X. China: awakening giant developing solutions to
2050. London: Alzheimers Disease International; 2013. Available from: www. population aging. Gerontologist. 2012 Oct;52(5):58996. doi: http://dx.doi.
alz.co.uk/research/GlobalImpactDementia2013.pdf [cited 2015 Apr 10]. org/10.1093/geront/gns105 PMID: 22936537
2. Zhang Y, Xu Y, Nie H, Lei T, Wu Y, Zhang L, et al. Prevalence of dementia 7. Wimo A, Jnsson L, Bond J, Prince M, Winblad B; Alzheimer Disease
and major dementia subtypes in the Chinese populations: a meta-analysis International. The worldwide economic impact of dementia 2010.
of dementia prevalence surveys, 19802010. J Clin Neurosci. 2012 Alzheimers Dement. 2013 Jan;9(1):111, e3.doi: http://dx.doi.org/10.1016/j.
Oct;19(10):13337.doi: http://dx.doi.org/10.1016/j.jocn.2012.01.029 PMID: jalz.2012.11.006 PMID: 23305821
22682650 8. Skldunger A, Wimo A, Johnell K. Net costs of dementia in Sweden an
3. Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, Car J, et al.; Global Health incidence based 10 year simulation study. Int J Geriatr Psychiatry. 2012
Epidemiology Reference Group (GHERG). Epidemiology of Alzheimers Nov;27(11):11127.doi: http://dx.doi.org/10.1002/gps.2828 PMID:
disease and other forms of dementia in China, 19902010: a systematic 22298311
review and analysis. Lancet. 2013 Jun 8;381(9882):201623.doi: http:// 9. Knapp M, Prince M. Dementia UK. London: Alzheimers Society; 2007.
dx.doi.org/10.1016/S0140-6736(13)60221-4 PMID: 23746902 Available from: www.alzheimers.org.uk/site/scripts/download_info.
4. Wu YT, Lee HY, Norton S, Prina AM, Fleming J, Matthews FE, et al. Period, php?fileID=2323 [cited 2015 Mar 12].
birth cohort and prevalence of dementia in mainland China, Hong Kong 10. Oremus M, Aguilar SC. A systematic review to assess the policy-making
and Taiwan: a meta-analysis. Int J Geriatr Psychiatry. 2014 Dec;29(12):1212 relevance of dementia cost-of-illness studies in the US and Canada.
20.doi: http://dx.doi.org/10.1002/gps.4148 PMID: 24854229 Pharmacoeconomics. 2011 Feb;29(2):14156.doi: http://dx.doi.
5. Jia J, Wang F, Wei C, Zhou A, Jia X, Li F, et al. The prevalence of dementia in org/10.2165/11539450-000000000-00000 PMID: 21090840
urban and rural areas of China. Alzheimers Dement. 2014 Jan;10(1):19. 11. Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of
PMID: 23871765 dementia in the United States. N Engl J Med. 2013 Apr 4;368(14):132634.
doi: http://dx.doi.org/10.1056/NEJMsa1204629 PMID: 23550670
Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726 25
Research
Economic burden of dementia in China Junfang Xu et al.
12. Olesen J, Gustavsson A, Svensson M, Wittchen HU, Jnsson B; CDBE2010 34. Wu C, Gao L, Chen S, Dong H. Care services for elderly people with
study group; European Brain Council. The economic cost of brain disorders dementia in rural China: a case study. Bull World Health Organ. 2016
in Europe. Eur J Neurol. 2012 Jan;19(1):15562. PMID: 22175760 Mar 1;94(3):16773.doi: http://dx.doi.org/10.2471/BLT.15.160929 PMID:
13. World Alzheimer Report 2010: the global economic impact of dementia. 26966327
London: Alzheimers Disease International; 2010. Available from: http:// 35. Wagstaff A, Yip W, Lindelow M, Hsiao WC. Chinas health system and its
www.alz.co.uk/research/files/WorldAlzheimerReport2010.pdf [cited 2015 reform: a review of recent studies. Health Econ. 2009 Jul;18(2) Suppl
Apr 21]. 2:S723. PMID: 19551753
14. The international statistical classification of diseases and related health 36. Bakker C, de Vugt ME, van Vliet D, Verhey FR, Pijnenburg YA, Vernooij-Dassen
problem, tenth revision. Geneva: World Health Organization; 1992. Available MJ, et al. The use of formal and informal care in early onset dementia: results
from: http://www.who.int/classifications/icd/en/ [cited 2015 Apr 21]. from the NeedYD study. Am J Geriatr Psychiatry. 2013 Jan;21(1):3745.
15. Wang G, Cheng Q, Zhang S, Bai L, Zeng J, Cui PJ, et al. Economic impact PMID: 23290201
of dementia in developing countries: an evaluation of Alzheimer-type 37. Jimnez-Martn S, Prieto CV. The trade-off between formal and informal
dementia in Shanghai, China. J Alzheimers Dis. 2008 Sep;15(1):10915. care in Spain. Eur J Health Econ. 2012 Aug;13(4):46190. PMID: 21584815
PMID: 18780971 38. Flaherty JH, Liu ML, Ding L, Dong B, Ding Q, Li X, et al. China: the aging
16. China statistical yearbook 2015. Beijing: National Bureau of Statistics of giant. J Am Geriatr Soc. 2007 Aug;55(8):1295300.doi: http://dx.doi.
China; 2015. Available from: http://www.stats.gov.cn/tjsj/ndsj/2015/ org/10.1111/j.1532-5415.2007.01273.x PMID: 17661972
indexeh.htm [cited 2015 Apr 21]. 39. Glass AP, Gao Y, Luo J. China: facing a long-term care challenge on an
17. United Nations Population Information Network [Internet]. New York: United unprecedented scale. Glob Public Health. 2013 Jul;8(6):72538. PMID:
Nations; 2015. Available from: www.un.org/popin [cited 2015 Apr 21]. 23600434
18. Chen LL, Zhao GM, Tang JK, Fang H. A study on the economic burden 40. Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational
of people with senile dementia in nursing homes. Chin Health Econ. interventions for informal caregivers of individuals with dementia residing
2009;28(11):1921. Chinese. in the community: systematic review and meta-analysis of randomised
19. Hu WS, Tang MN, Zheng HB, Ma C, Hu HY. Study on economic burden of controlled trials. Int J Geriatr Psychiatry. 2015 Feb;30(2):13043.doi: http://
senile dementia in community, nursing institution and psychiatric hospital. dx.doi.org/10.1002/gps.4208 PMID: 25354132
J Pract Med. 2008;24(10):18213. Chinese. 41. Qiu C, Fratiglioni L. A major role for cardiovascular burden in age-related
20. Wang H, Gao TF, Wimo A, Yu X. Caregiver time and cost of home care for cognitive decline. Nat Rev Cardiol. 2015 May;12(5):26777.doi: http://dx.doi.
Alzheimers disease: a clinic-based observational study in Beijing, China. Ageing org/10.1038/nrcardio.2014.223 PMID: 25583619
Int. 2010;35(2):15365. doi: http://dx.doi.org/10.1007/s12126-010-9056-1 42. Qiu C, von Strauss E, Bckman L, Winblad B, Fratiglioni L. Twenty-year
21. Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al. Prevalence, changes in dementia occurrence suggest decreasing incidence in central
treatment, and associated disability of mental disorders in four provinces Stockholm, Sweden. Neurology. 2013 May 14;80(20):188894.doi: http://
in China during 200105: an epidemiological survey. Lancet. 2009 dx.doi.org/10.1212/WNL.0b013e318292a2f9 PMID: 23596063
Jun 13;373(9680):204153.doi: http://dx.doi.org/10.1016/S0140- 43. Matthews FE, Stephan BC, Robinson L, Jagger C, Barnes LE, Arthur A, et al.;
6736(09)60660-7 PMID: 19524780 Cognitive Function and Ageing Studies (CFAS) Collaboration. A two decade
22. Reisberg B, Ferris SH, de Leon MJ, Crook T. The Global Deterioration Scale dementia incidence comparison from the Cognitive Function and Ageing
for assessment of primary degenerative dementia. Am J Psychiatry. 1982 Studies I and II. Nat Commun. 2016;7:11398.doi: http://dx.doi.org/10.1038/
Sep;139(9):11369. doi: http://dx.doi.org/10.1176/ajp.139.9.1136 PMID: ncomms11398 PMID: 27092707
7114305 44. Satizabal CL, Beiser AS, Chouraki V, Chne G, Dufouil C, Seshadri S. Incidence
23. Li H, Huang PR. The disability weights and burden of inpatients with of dementia over three decades in the Framingham Heart Study. N
dementia. Chin J Gerontol. 2010;30:2435. Chinese. Engl J Med. 2016 Feb 11;374(6):52332.doi: http://dx.doi.org/10.1056/
24. Luengo-Fernandez R, Leal J, Gray A, Sullivan R. Economic burden of cancer NEJMoa1504327 PMID: 26863354
across the European Union: a population-based cost analysis. Lancet 45. Winblad B, Amouyel P, Andrieu S, Ballard C, Brayne C, Brodaty H, et al.
Oncol. 2013 Nov;14(12):116574.doi: http://dx.doi.org/10.1016/S1470- Defeating Alzheimers disease and other dementias: a priority for European
2045(13)70442-X PMID: 24131614 science and society. Lancet Neurol. 2016 Apr;15(5):455532. PMID:
25. Ruwaard D, Hoogenveen RT, Verkleij H, Kromhout D, Casparie AF, van der 26987701
Veen EA. Forecasting the number of diabetic patients in the Netherlands 46. Dixon J, Ferdinand M, DAmico F, Knapp M. Exploring the cost-effectiveness
in 2005. Am J Public Health. 1993 Jul;83(7):98995.doi: http://dx.doi. of a one-off screen for dementia (for people aged 75 years in England and
org/10.2105/AJPH.83.7.989 PMID: 8328622 Wales). Int J Geriatr Psychiatry. 2015 May;30(5):44652.doi: http://dx.doi.
26. Ang BW. Decomposition analysis for policymaking in energy: which is the org/10.1002/gps.4158 PMID: 25043227
preferred method? Energy Policy. 2004;32(9):11319. doi: http://dx.doi. 47. Brayne C, Fox C, Boustani M. Dementia screening in primary care: is it time?
org/10.1016/S0301-4215(03)00076-4 JAMA. 2007 Nov 28;298(20):240911. PMID: 18042918
27. Cheng XM. Health economics. 2nd ed. Beijing: Peoples Medical Publishing 48. Banerjee S, Wittenberg R. Clinical and cost effectiveness of services for
House; 2007. p. 90. Chinese. early diagnosis and intervention in dementia. Int J Geriatr Psychiatry. 2009
28. Corrada MM, Brookmeyer R, Berlau D, Paganini-Hill A, Kawas CH. Prevalence Jul;24(7):74854. PMID: 19206079
of dementia after age 90: results from the 90+ study. Neurology. 2008 Jul 49. Xu J, Wang J, Wimo A, Qiu C. The economic burden of mental disorders
29;71(5):33743.doi: http://dx.doi.org/10.1212/01.wnl.0000310773.65918. in China, 20052013: implications for health policy. BMC Psychiatry.
cd PMID: 18596243 2016;16(1):137.doi: http://dx.doi.org/10.1186/s12888-016-0839-0 PMID:
29. Lucca U, Tettamanti M, Logroscino G, Tiraboschi P, Landi C, Sacco L, et al. 27169936
Prevalence of dementia in the oldest old: the Monzino 80-plus population 50. Bunn F, Burn AM, Goodman C, Rait G, Norton S, Robinson L, et al.
based study. Alzheimers Dement. 2015 Mar;11(3):25870.e3. PMID: Comorbidity and dementia: a scoping review of the literature. BMC Med.
25150732 2014;12:192. PMID: 25358236
30. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, et al. Rapid health 51. Poblador-Plou B, Caldern-Larraaga A, Marta-Moreno J, Hancco-Saavedra
transition in China, 19902010: findings from the Global Burden of Disease J, Sicras-Mainar A, Soljak M, et al. Comorbidity of dementia: a cross-sectional
Study 2010. Lancet. 2013 Jun 8;381(9882):19872015. PMID: 23746901 study of primary care older patients. BMC Psychiatry. 2014;14(1):84.doi:
31. Schaller S, Mauskopf J, Kriza C, Wahlster P, Kolominsky-Rabas PL. The main http://dx.doi.org/10.1186/1471-244X-14-84 PMID: 24645776
cost drivers in dementia: a systematic review. Int J Geriatr Psychiatry. 2015 52. Brookmeyer R, Evans DA, Hebert L, Langa KM, Heeringa SG, Plassman BL,
Feb;30(2):11129.doi: http://dx.doi.org/10.1002/gps.4198 PMID: 25320002 et al. National estimates of the prevalence of Alzheimers disease in the
32. Dementia: a public health priority. Geneva: World Health Organization; United States. Alzheimers Dement. 2011 Jan;7(1):6173.doi: http://dx.doi.
2012. Available from: http://www.who.int/mental_health/publications/ org/10.1016/j.jalz.2010.11.007 PMID: 21255744
dementia_report_2012/en/ [cited 2015 Apr 21]. 53. Norton S, Matthews FE, Brayne C. A commentary on studies presenting
33. Zhu CW, Scarmeas N, Torgan R, Albert M, Brandt J, Blacker D, et al. projections of the future prevalence of dementia. BMC Public Health.
Clinical features associated with costs in early AD: baseline data from the 2013;13(1):1. PMID: 23280303
Predictors Study. Neurology. 2006 Apr 11;66(7):10218.doi: http://dx.doi.
org/10.1212/01.wnl.0000204189.18698.c7 PMID: 16606913
26 Bull World Health Organ 2017;95:1826| doi: http://dx.doi.org/10.2471/BLT.15.167726
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Sample Q and AДокумент47 страницSample Q and AHareesha N G100% (1)
- Shareholders AgreementДокумент12 страницShareholders Agreementmetareason100% (1)
- Virginia's Rare Animals GuideДокумент83 страницыVirginia's Rare Animals Guidezineil BlackwoodОценок пока нет
- Probability 2Документ5 страницProbability 2shadowosОценок пока нет
- Service and Repair ManualДокумент373 страницыService and Repair ManualrunolevariОценок пока нет
- Knowledge Management in Smes and MNCS: Matching Knowledge Mobility Mechanisms To Supply Network Configuration ProfilesДокумент25 страницKnowledge Management in Smes and MNCS: Matching Knowledge Mobility Mechanisms To Supply Network Configuration Profilessalsabila fitristantiОценок пока нет
- DBL PDFДокумент5 страницDBL PDFfiatauroОценок пока нет
- Bader and Overton CompetitionДокумент4 страницыBader and Overton CompetitionJulien SiinoОценок пока нет
- KBCДокумент3 страницыKBCjoydurgaОценок пока нет
- Manual Multilin 369Документ290 страницManual Multilin 369Jesus Landaeta100% (1)
- Intelligent Traffic Management Using SDNДокумент5 страницIntelligent Traffic Management Using SDNEngr XsadОценок пока нет
- By: Rupesh RavaniДокумент28 страницBy: Rupesh RavaniNguyễn Hoàng ThànhОценок пока нет
- One-Point Perspective and Other Renaissance Ideas in Gentile Da Fabriano's 'The Presentation of Christ in The Temple' From 'The Strozzi Altarpiece', 1423Документ46 страницOne-Point Perspective and Other Renaissance Ideas in Gentile Da Fabriano's 'The Presentation of Christ in The Temple' From 'The Strozzi Altarpiece', 1423RОценок пока нет
- Spirit Mandala CrochetДокумент5 страницSpirit Mandala CrochetViviana CastilloОценок пока нет
- Hematopoiesis, Including Lymphocyte Development and MaturationДокумент2 страницыHematopoiesis, Including Lymphocyte Development and MaturationMuhammad FakhrizalОценок пока нет
- Conference Pamphlet English Version (2) - 1Документ3 страницыConference Pamphlet English Version (2) - 1AdelОценок пока нет
- BNPL ReportДокумент38 страницBNPL Reportvishu kОценок пока нет
- Chase. The Lord's Prayer in The Early Church. 1891.Документ200 страницChase. The Lord's Prayer in The Early Church. 1891.Patrologia Latina, Graeca et Orientalis100% (3)
- The Complete Android User Manual (21st Ed.,2024)Документ142 страницыThe Complete Android User Manual (21st Ed.,2024)George_200Оценок пока нет
- CPWD RatesДокумент197 страницCPWD RatespnkjinamdarОценок пока нет
- Sophia Perennis As A Means of SalvationДокумент12 страницSophia Perennis As A Means of SalvationJoranxxxОценок пока нет
- UTS Business Statistics: Skewerness, Probability and Some BinomialДокумент6 страницUTS Business Statistics: Skewerness, Probability and Some BinomialemilyОценок пока нет
- Sriman NarayaneeyamДокумент280 страницSriman NarayaneeyamSharma Joshi100% (1)
- مفاتح الفرجДокумент209 страницمفاتح الفرجBuya Munawwir al-QosimiОценок пока нет
- Ford v. West, 10th Cir. (1998)Документ9 страницFord v. West, 10th Cir. (1998)Scribd Government DocsОценок пока нет
- A Seminar Report On: "Wireless Charging"Документ36 страницA Seminar Report On: "Wireless Charging"shreyarai2167% (6)
- PolymersДокумент8 страницPolymersLauren LloydОценок пока нет
- RAICES LawsuitДокумент25 страницRAICES LawsuitJohn MoritzОценок пока нет
- Operation and Marketing ManagerДокумент5 страницOperation and Marketing ManagerMukesh RaiyaОценок пока нет
- HYSTER H4.0UT, H4.5UT, H5.0UT PARTS MANUALconvДокумент162 страницыHYSTER H4.0UT, H4.5UT, H5.0UT PARTS MANUALconvNoufou OuedraogoОценок пока нет