Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- TK102 User ManualДокумент12 страницTK102 User ManualfjpaОценок пока нет
- Engineer: Ergonomic Is ConcernedДокумент17 страницEngineer: Ergonomic Is ConcernedKhuda BukshОценок пока нет
- Spot Light: Spo2 Functional TesterДокумент28 страницSpot Light: Spo2 Functional TesterMasimo RootОценок пока нет
- Technical Manual For Float Cum Boost Battery Charger (S1A02)Документ8 страницTechnical Manual For Float Cum Boost Battery Charger (S1A02)DEEPAKОценок пока нет
- BSNL GPON A/T ScheduleДокумент8 страницBSNL GPON A/T Scheduleman_i_acОценок пока нет
- Pakistan SRO V.ruling 2015Документ62 страницыPakistan SRO V.ruling 2015Abid AliОценок пока нет
- Specification: Constant Current Discharge Characteristics: A (25)Документ2 страницыSpecification: Constant Current Discharge Characteristics: A (25)GeorgeОценок пока нет
- AC5!02!05 Aionic en EspañolДокумент24 страницыAC5!02!05 Aionic en EspañolAlex PqОценок пока нет
- SUA3000RMXL3UДокумент22 страницыSUA3000RMXL3Ua.elwahabОценок пока нет
- Soleus GPSOne Manual 080615Документ3 страницыSoleus GPSOne Manual 080615markanthony_alvario2946Оценок пока нет
- EFFTRONICS Battery Health Monitoring SystemДокумент2 страницыEFFTRONICS Battery Health Monitoring SystemJorge MonteiroОценок пока нет
- SIM300D: Hardware SpecificationДокумент53 страницыSIM300D: Hardware Specificationescu_escuОценок пока нет
- TowFLEXX® 600 RCДокумент12 страницTowFLEXX® 600 RCAREZZO AVIAОценок пока нет
- Efr52 Cut SheetДокумент1 страницаEfr52 Cut Sheetmike00Оценок пока нет
- CAT Battery Quick Reference GuideДокумент2 страницыCAT Battery Quick Reference GuidemkОценок пока нет
- 99inspectestform PDFДокумент4 страницы99inspectestform PDFamaljacobОценок пока нет
- MM850242-3 MicroCal PДокумент54 страницыMM850242-3 MicroCal Pctmtectrol100% (1)
- C7x00 C-Series BrochureДокумент8 страницC7x00 C-Series BrochurecristiОценок пока нет
- Manual: M57x Bitronics Compact IEDДокумент110 страницManual: M57x Bitronics Compact IEDMikeОценок пока нет
- 2012 - 13 Fuel Cells For Ships PDFДокумент20 страниц2012 - 13 Fuel Cells For Ships PDFteriaxОценок пока нет
- Aircraft Battery Component Maintenance ManualДокумент60 страницAircraft Battery Component Maintenance ManualPaNos P Ami100% (2)
- Batería PowerSafe - Front Terminal - Range SummaryДокумент2 страницыBatería PowerSafe - Front Terminal - Range SummaryFranco CortezОценок пока нет
- Bomba SKC 222 ManualДокумент11 страницBomba SKC 222 ManualEderson GuimaraesОценок пока нет
- Solar Charger User Manual - 20210729 - 0001Документ2 страницыSolar Charger User Manual - 20210729 - 0001gohsaikitОценок пока нет
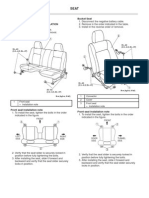
- Bucket Seat: 1 Connector 2 Cover 3 Front Seat Installation NoteДокумент7 страницBucket Seat: 1 Connector 2 Cover 3 Front Seat Installation Notepavel35Оценок пока нет
- Batteryrpt2011NissanLeaf0356 NissanДокумент17 страницBatteryrpt2011NissanLeaf0356 NissanAleksandra Radovanovic100% (1)
- Electrochemistry 1Документ62 страницыElectrochemistry 1Jane DocdocОценок пока нет
- GP0001Документ12 страницGP0001mdasifkhan2013Оценок пока нет
- Minipack, PS System: Quick Start GuideДокумент40 страницMinipack, PS System: Quick Start GuidemiskoyuОценок пока нет