Вам также может понравиться
- Neurotransmitters and Psychotropic MedicationsДокумент8 страницNeurotransmitters and Psychotropic MedicationsDale Buckman100% (1)
- Decision TreeДокумент185 страницDecision TreeNathan D. Croy50% (2)
- Fusion Tech ActДокумент74 страницыFusion Tech ActrahulrsinghОценок пока нет
- Psychopharmacology Chapter on Classification, Mechanisms, and Effects of Antipsychotic, Antidepressant, and Antimanic DrugsДокумент18 страницPsychopharmacology Chapter on Classification, Mechanisms, and Effects of Antipsychotic, Antidepressant, and Antimanic DrugsDrima EdiОценок пока нет
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsДокумент9 страницPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyОценок пока нет
- Code of Conduct GuidanceДокумент17 страницCode of Conduct GuidanceMuhammad RidwanОценок пока нет
- Antipsychotic DrugsДокумент44 страницыAntipsychotic DrugsPaulus Widjanarko Brotosaputro0% (1)
- Drug List PsychopharmДокумент23 страницыDrug List PsychopharmGeorge HananiaОценок пока нет
- Psychotherapeutic Drugs GuideДокумент12 страницPsychotherapeutic Drugs Guidecamile buhanginОценок пока нет
- Antipsychotics Guide for Nursing Intervention and Patient EducationДокумент10 страницAntipsychotics Guide for Nursing Intervention and Patient Educationwawing16Оценок пока нет
- Psychotropics NotesДокумент5 страницPsychotropics NotesJulianna Rheaven JoreОценок пока нет
- Of Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart FailureДокумент31 страницаOf Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart Failurenaikram420Оценок пока нет
- Drug ListДокумент30 страницDrug ListKristineОценок пока нет
- Psych DrugsДокумент3 страницыPsych DrugsSwarna BanikОценок пока нет
- Drug List LongДокумент17 страницDrug List Long林鹿兒Оценок пока нет
- Psych Drugs List - To Be Filled inДокумент3 страницыPsych Drugs List - To Be Filled inM Patel100% (1)
- Mnemonics PDFДокумент10 страницMnemonics PDFود امدرОценок пока нет
- Drug ClassДокумент13 страницDrug ClassEdfren Salazar Colon100% (1)
- ANTIPSYCHOTICS Olanzapine (Zyprexa), Aripiprazole (Abilify), Chlorpromazine (Thorazine)Документ5 страницANTIPSYCHOTICS Olanzapine (Zyprexa), Aripiprazole (Abilify), Chlorpromazine (Thorazine)Rhanne BolanteОценок пока нет
- Module 1 - IntroductionДокумент30 страницModule 1 - Introductionpsychopharmacology100% (2)
- Behavioral Health Medication ListДокумент1 страницаBehavioral Health Medication ListAndrew Harrison LewisОценок пока нет
- ANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsДокумент21 страницаANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsKashis SharmaОценок пока нет
- Antimanic DrugsДокумент22 страницыAntimanic DrugsMarlet N. Ortega100% (2)
- Psychiatry: AntidepressantsДокумент2 страницыPsychiatry: AntidepressantsSok-Moi Chok100% (1)
- Pharmacotherapy in PschiatryДокумент8 страницPharmacotherapy in PschiatryygfhdgОценок пока нет
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Документ48 страницNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanОценок пока нет
- Therapeutic Drug MonitoringДокумент10 страницTherapeutic Drug MonitoringAnnie SethiОценок пока нет
- Pharm TableДокумент35 страницPharm TableHannah BaldwinОценок пока нет
- Pharmacology (1) - 104-122Документ19 страницPharmacology (1) - 104-122Dental LecturesMMQОценок пока нет
- Adjuvant AnalgesicsДокумент44 страницыAdjuvant AnalgesicsZulfan EfendiОценок пока нет
- CNS Depressants and Muscle RelaxantsДокумент23 страницыCNS Depressants and Muscle RelaxantsSV SagarОценок пока нет
- Drugs Drugs Drugs STUDY GUIDEДокумент13 страницDrugs Drugs Drugs STUDY GUIDEAlexander Chamessian100% (1)
- Buku Comprehensive Textbook PsychiatryДокумент76 страницBuku Comprehensive Textbook PsychiatryHadi GunaОценок пока нет
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsДокумент29 страницPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaОценок пока нет
- Gout DrugsДокумент1 страницаGout DrugsMichael BrownОценок пока нет
- PA 644 - M2 LecturesДокумент412 страницPA 644 - M2 LectureskatОценок пока нет
- ANP Masters Qualifications RolesДокумент4 страницыANP Masters Qualifications RolesN.DanielaОценок пока нет
- Drugs Acting on Autonomic Nervous SystemДокумент72 страницыDrugs Acting on Autonomic Nervous SystemDebashis ParidaОценок пока нет
- Asthma & COPD Medication List PDFДокумент11 страницAsthma & COPD Medication List PDFabdullah992011Оценок пока нет
- Patient Assessment FormДокумент10 страницPatient Assessment FormAdam GОценок пока нет
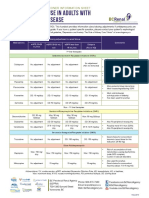
- Antidepressant Use in Adults With Chronic Kidney DiseaseДокумент1 страницаAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Psychiatric Interview Module 1Документ41 страницаPsychiatric Interview Module 1Spj Bernardo100% (1)
- Psychopharmacology Mnemonics for Antidepressants, Anticonvulsants, Anti-anxiety DrugsДокумент21 страницаPsychopharmacology Mnemonics for Antidepressants, Anticonvulsants, Anti-anxiety DrugsJoseph Rommel Castro CortezОценок пока нет
- Non-Opioid Analgesics and Types of AnesthesiaДокумент31 страницаNon-Opioid Analgesics and Types of AnesthesiaIvonnie Mae MaeОценок пока нет
- Treatment Modalities For Mood DisordersДокумент55 страницTreatment Modalities For Mood DisordersGlory MimiОценок пока нет
- Antimanic DrugsДокумент9 страницAntimanic DrugscradletalkОценок пока нет
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsДокумент3 страницыDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinОценок пока нет
- PSYCH - MBBS - (Use Outline To Create Other Templates) Anggelos NotesДокумент26 страницPSYCH - MBBS - (Use Outline To Create Other Templates) Anggelos NotesNariska Cooper100% (2)
- PHARMACOLOGY OF PSYCHOSIS AND MANIAДокумент53 страницыPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaОценок пока нет
- NHS Antibiotice PDFДокумент2 страницыNHS Antibiotice PDFHoratiu OanaОценок пока нет
- Psych Ch. 7 Notes (Tutor)Документ5 страницPsych Ch. 7 Notes (Tutor)Haylle ThomasОценок пока нет
- Current Clinical Strategies: Handbook of Psychiatric DrugsДокумент72 страницыCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Оценок пока нет
- Ketamine For Opiate WithdrawalДокумент3 страницыKetamine For Opiate WithdrawalroboОценок пока нет
- Psychotropic MedicationsДокумент87 страницPsychotropic MedicationsDWAI McJohnsonОценок пока нет
- ABCs of Psychiatric MedicinesДокумент41 страницаABCs of Psychiatric Medicines아이닠텓Оценок пока нет
- Renal Guide and Charts: AlbuminДокумент16 страницRenal Guide and Charts: AlbuminYaima JimenezОценок пока нет
- Understanding Antipsychotic DrugsДокумент22 страницыUnderstanding Antipsychotic DrugsvinodksahuОценок пока нет
- LECTURE 22: Antipsychotic Agents & Lithium: OutlineДокумент5 страницLECTURE 22: Antipsychotic Agents & Lithium: OutlineRosa PalconitОценок пока нет
- Overview of Psychotropic DrugsДокумент7 страницOverview of Psychotropic Drugsnad101Оценок пока нет
- نسخة Antidepressants for Lab. StudentsДокумент64 страницыنسخة Antidepressants for Lab. Studentsنوف الحربي.Оценок пока нет
- Blunted Affect: Manic EpisodesДокумент1 страницаBlunted Affect: Manic EpisodesSofia Centro TaerОценок пока нет
- Code of Ethics For Philippine PsychologistsДокумент28 страницCode of Ethics For Philippine PsychologistsPamela Lite100% (1)
- Mental Health StatsДокумент8 страницMental Health StatsSofia Centro TaerОценок пока нет
- A. Administration: File No. TitleДокумент2 страницыA. Administration: File No. TitleSofia Centro TaerОценок пока нет
- Promissory NoteДокумент1 страницаPromissory NoteSofia Centro TaerОценок пока нет
- SnowflakesДокумент1 страницаSnowflakesSofia Centro TaerОценок пока нет
- QAДокумент2 страницыQASofia Centro TaerОценок пока нет
- Chocolate Crinkles & Chewy Chocolate Chip Cookies RecipeДокумент1 страницаChocolate Crinkles & Chewy Chocolate Chip Cookies RecipeSofia Centro TaerОценок пока нет
- Saint Thomas Aquinas Prayer Before StudyДокумент1 страницаSaint Thomas Aquinas Prayer Before StudySofia Centro TaerОценок пока нет
- What Is Mental HealthДокумент23 страницыWhat Is Mental HealthSofia Centro Taer100% (1)
- Rights of A ChildДокумент16 страницRights of A ChildSofia Centro TaerОценок пока нет
- HappybirthdayДокумент3 страницыHappybirthdaySofia Centro TaerОценок пока нет
- CharadesДокумент3 страницыCharadesSofia Centro TaerОценок пока нет
- Importance of Written CommunicationДокумент8 страницImportance of Written CommunicationSofia Centro TaerОценок пока нет
- Gregor Mendel's Groundbreaking Discoveries in GeneticsДокумент35 страницGregor Mendel's Groundbreaking Discoveries in GeneticsSofia Centro TaerОценок пока нет
- The Urinary SystemДокумент26 страницThe Urinary SystemSofia Centro TaerОценок пока нет
- Conformity ExperimentДокумент3 страницыConformity ExperimentSofia Centro TaerОценок пока нет
- Letter To The LibraryДокумент2 страницыLetter To The LibrarySofia Centro TaerОценок пока нет
- FungiДокумент49 страницFungiSofia Centro TaerОценок пока нет
- Importance of Written CommunicationДокумент8 страницImportance of Written CommunicationSofia Centro TaerОценок пока нет
- Guidance and CounselingДокумент10 страницGuidance and CounselingSofia Centro TaerОценок пока нет
- Sun Magic Zone Call and Text UnlimitedДокумент1 страницаSun Magic Zone Call and Text UnlimitedSofia Centro TaerОценок пока нет
- Filipino Philosophy DДокумент1 страницаFilipino Philosophy DSofia Centro TaerОценок пока нет
- Sun Magic Zone Call and Text UnlimitedДокумент1 страницаSun Magic Zone Call and Text UnlimitedSofia Centro TaerОценок пока нет
- Chapter 5 Quiz Corrections AДокумент4 страницыChapter 5 Quiz Corrections Aapi-244140508Оценок пока нет
- ISE I Conversation Task - Rules and RegulationsДокумент3 страницыISE I Conversation Task - Rules and RegulationsElena B. HerreroОценок пока нет
- VDA ChinaДокумент72 страницыVDA Chinatuananh1010Оценок пока нет
- Method of IstinjaДокумент24 страницыMethod of IstinjaIslamic LibraryОценок пока нет
- Henderson - Historical Documents of The Middle AgesДокумент536 страницHenderson - Historical Documents of The Middle AgesVlad VieriuОценок пока нет
- SOLUS Is An Autonomous System That Enables Hyper-Personalized Engagement With Individual Customers at ScaleДокумент3 страницыSOLUS Is An Autonomous System That Enables Hyper-Personalized Engagement With Individual Customers at ScaleShikhaОценок пока нет
- Untitled DocumentДокумент2 страницыUntitled DocumentClaudia WinОценок пока нет
- Perkin Elmer Singapore Distribution CaseДокумент3 страницыPerkin Elmer Singapore Distribution CaseJackie Canlas100% (1)
- CBCP Monitor Vol. 17 No. 9Документ20 страницCBCP Monitor Vol. 17 No. 9Areopagus Communications, Inc.Оценок пока нет
- Japanese Tea Cups LessonДокумент3 страницыJapanese Tea Cups Lessonapi-525048974Оценок пока нет
- Report-Picic & NibДокумент18 страницReport-Picic & NibPrincely TravelОценок пока нет
- Geometry Solving Problems (Circles)Документ36 страницGeometry Solving Problems (Circles)Hero MirasolОценок пока нет
- 3B Adverbial PhrasesДокумент1 страница3B Adverbial PhrasesSarah IОценок пока нет
- The City - Populus' As A Self-Governing CorporationДокумент24 страницыThe City - Populus' As A Self-Governing Corporation马寅秋Оценок пока нет
- DRR Module 4 Detailed Lesson PlanДокумент8 страницDRR Module 4 Detailed Lesson PlanFe Annalie Sacal100% (2)
- FunambolДокумент48 страницFunambolAmeliaОценок пока нет
- June 2016 - QuestionsДокумент8 страницJune 2016 - Questionsnasir_m68Оценок пока нет
- Kung Fu MedicinesДокумент9 страницKung Fu MedicinesDavid HewittОценок пока нет
- Primer To Using Stampplot® Pro Standard User LicensedДокумент21 страницаPrimer To Using Stampplot® Pro Standard User LicensedSandy Rachman AdrianОценок пока нет
- Chapter 11, 12 Curve Tracing and EnvelopeДокумент37 страницChapter 11, 12 Curve Tracing and EnvelopeNitish PokhrelОценок пока нет
- Liquid Hydrogen As A Propulsion Fuel, 1945-1959Документ341 страницаLiquid Hydrogen As A Propulsion Fuel, 1945-1959Bob AndrepontОценок пока нет
- Evelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"Документ44 страницыEvelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"s0metim3sОценок пока нет
- Crossing To The Dark Side:: Examining Creators, Outcomes, and Inhibitors of TechnostressДокумент9 страницCrossing To The Dark Side:: Examining Creators, Outcomes, and Inhibitors of TechnostressVentas FalcónОценок пока нет
- Benefits and Risks of Dexamethasone in Noncardiac Surgery: Clinical Focus ReviewДокумент9 страницBenefits and Risks of Dexamethasone in Noncardiac Surgery: Clinical Focus ReviewAlejandra VillaОценок пока нет
- International Marketing ModuleДокумент131 страницаInternational Marketing ModuleTekle KochitoОценок пока нет
- Carb-Based-Dll No. 2 - 4th Qtr.Документ5 страницCarb-Based-Dll No. 2 - 4th Qtr.Kathrene Santos RiveraОценок пока нет
- The Republic of LOMAR Sovereignty and International LawДокумент13 страницThe Republic of LOMAR Sovereignty and International LawRoyalHouseofRA UruguayОценок пока нет
- General Ledger Journal Import ProcessДокумент13 страницGeneral Ledger Journal Import ProcessMadhavi SinghОценок пока нет