Вам также может понравиться
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationДокумент6 страницAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonОценок пока нет
- Drugs For NeurolepticsДокумент1 страницаDrugs For Neurolepticssyamil_daudОценок пока нет
- 504 - Pediatric Psychopharmacology - General PrinciplesДокумент54 страницы504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroОценок пока нет
- PSYC - Medication TemplateДокумент15 страницPSYC - Medication TemplateM Henry100% (1)
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPДокумент33 страницыIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Pharmacology - (5) Psychotic DrugsДокумент8 страницPharmacology - (5) Psychotic DrugsSamantha DiegoОценок пока нет
- Mental Status Examination Rapid Record Form: CatatoniaДокумент3 страницыMental Status Examination Rapid Record Form: CatatoniaNicole TangcoОценок пока нет
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeОт EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeОценок пока нет
- Adhd Toolkit MedicationsДокумент1 страницаAdhd Toolkit MedicationsreneezОценок пока нет
- SSRI (Selective Serotonin Reuptake Inhibitor)Документ1 страницаSSRI (Selective Serotonin Reuptake Inhibitor)Mike EveretteОценок пока нет
- History of Presenting ComplaintДокумент2 страницыHistory of Presenting ComplaintAnne SisonОценок пока нет
- Just Getting The Main RX Names Down : Antidepressants Mood StabilizersДокумент1 страницаJust Getting The Main RX Names Down : Antidepressants Mood StabilizersCarlos Eduardo LinaresОценок пока нет
- Shortened REM Latency and Increased REM: Previous AttemptДокумент19 страницShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenОценок пока нет
- Workplace Violence PreventionДокумент12 страницWorkplace Violence PreventionAnuraj SrivastavaОценок пока нет
- Antipsychotics Guide for Nursing Intervention and Patient EducationДокумент10 страницAntipsychotics Guide for Nursing Intervention and Patient Educationwawing16Оценок пока нет
- Bipolar DisorderДокумент1 страницаBipolar DisorderNur BalqisОценок пока нет
- PSYCHOPHARMACOLOGYДокумент2 страницыPSYCHOPHARMACOLOGYJulia Rae Delos SantosОценок пока нет
- Mental Status Exam ChecklistДокумент6 страницMental Status Exam ChecklistainstusharОценок пока нет
- Role of Vitamin D in Schizophrenia in Elderly PatientДокумент3 страницыRole of Vitamin D in Schizophrenia in Elderly PatientJAVED ATHER SIDDIQUIОценок пока нет
- PMH Nursing GuideДокумент11 страницPMH Nursing Guidejwasylow13Оценок пока нет
- PsychiatryДокумент92 страницыPsychiatrykimОценок пока нет
- Psychopharmacology in Medically Ill PatientsДокумент21 страницаPsychopharmacology in Medically Ill PatientsAklile TsegaОценок пока нет
- Mse NotesДокумент25 страницMse NotesKevin Jaya SОценок пока нет
- Psychotropics NotesДокумент5 страницPsychotropics NotesJulianna Rheaven JoreОценок пока нет
- History TakingДокумент34 страницыHistory TakingSulieman MazahrehОценок пока нет
- Common Psychiatric MedicationsДокумент1 страницаCommon Psychiatric MedicationsDan Kiarie92% (12)
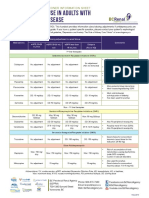
- Antidepressant Use in Adults With Chronic Kidney DiseaseДокумент1 страницаAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Patient Seeking Medically Supervised WithdrawalДокумент3 страницыPatient Seeking Medically Supervised WithdrawalLauren EОценок пока нет
- Psych Ch. 7 Notes (Tutor)Документ5 страницPsych Ch. 7 Notes (Tutor)Haylle ThomasОценок пока нет
- Final Capstone PaperДокумент15 страницFinal Capstone Paperapi-478784238Оценок пока нет
- Geriatric Giants - DR SeymourДокумент108 страницGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Sudden Onset (Within 2 Weeks) of at Least One of TheДокумент2 страницыSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaОценок пока нет
- Psych Ch. 5 NotesДокумент7 страницPsych Ch. 5 NotesHaylle ThomasОценок пока нет
- Generics Antidepressants Comparison Chart PDFДокумент2 страницыGenerics Antidepressants Comparison Chart PDFYazirОценок пока нет
- Buku Comprehensive Textbook PsychiatryДокумент76 страницBuku Comprehensive Textbook PsychiatryHadi GunaОценок пока нет
- Common Psychiatric TermsДокумент6 страницCommon Psychiatric TermsKatrina Heart Rauto AvilaОценок пока нет
- Mood and Psychotic Disorders GuideДокумент1 страницаMood and Psychotic Disorders GuideJeremy-ann HamОценок пока нет
- PMHNP Case Study Diagnosis and TreatmentДокумент7 страницPMHNP Case Study Diagnosis and TreatmentSoumyadeep BoseОценок пока нет
- Drug List PsychopharmДокумент23 страницыDrug List PsychopharmGeorge HananiaОценок пока нет
- Final FY Presentation1Документ45 страницFinal FY Presentation1SamОценок пока нет
- ANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsДокумент21 страницаANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsKashis SharmaОценок пока нет
- Anxiety/Depression: S AlprazolamДокумент2 страницыAnxiety/Depression: S AlprazolamleesaОценок пока нет
- 10 Cognitive DisordersДокумент16 страниц10 Cognitive DisordersFarrah MaeОценок пока нет
- Neuroanatomy For The Psychiatrist: Textbook of PsychiatryДокумент37 страницNeuroanatomy For The Psychiatrist: Textbook of Psychiatrykrysdana22Оценок пока нет
- n597 Psychiatric EvalДокумент11 страницn597 Psychiatric Evalapi-532870494Оценок пока нет
- Provisional: Borderline Personality Disorder Differential DXДокумент6 страницProvisional: Borderline Personality Disorder Differential DXhernandez2812Оценок пока нет
- Psychiatry Capstone 43020 Agitation PsychopharmacologyДокумент20 страницPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Оценок пока нет
- Antipsychotic DrugsДокумент54 страницыAntipsychotic DrugsJackОценок пока нет
- Delirium, Dementia, PsychosisДокумент2 страницыDelirium, Dementia, PsychosisLagente EstalocaОценок пока нет
- Algorithm for Treating DepressionДокумент12 страницAlgorithm for Treating Depressioniwul kiwul KriwulОценок пока нет
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Документ3 страницыHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaОценок пока нет
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiДокумент47 страницNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanОценок пока нет
- Psychiatry Case LogДокумент6 страницPsychiatry Case Logf3er3Оценок пока нет
- PSYCH 1.2A Mood DisordersДокумент22 страницыPSYCH 1.2A Mood DisordersZazaОценок пока нет
- History Taking and Mental State Exam for PsychosisДокумент10 страницHistory Taking and Mental State Exam for PsychosisNathan T. CheungОценок пока нет
- Laboratory Testing in PsychiatryДокумент29 страницLaboratory Testing in PsychiatrySera ChunОценок пока нет
- Open Fracture Classification and ManagementДокумент19 страницOpen Fracture Classification and ManagementnabiellarifinОценок пока нет
- Sudden Trauma: Overlying Skin IntactДокумент4 страницыSudden Trauma: Overlying Skin IntactSuha AbdullahОценок пока нет
- Basic Bone Fractures HandoutДокумент5 страницBasic Bone Fractures HandoutMuhammad HassanОценок пока нет
- Clearing The Cervical Spine: DR Claudia AY Cheng Senior Medical Officer Department of Anaesthesia and Intensive CareДокумент78 страницClearing The Cervical Spine: DR Claudia AY Cheng Senior Medical Officer Department of Anaesthesia and Intensive CareVictor ChanОценок пока нет
- Optics and Refraction For Podcast - David HunterДокумент74 страницыOptics and Refraction For Podcast - David HunterTiffany Fuentes100% (2)
- APCH 1024aДокумент7 страницAPCH 1024aVictor ChanОценок пока нет
- Chap 4 Part IIIДокумент3 страницыChap 4 Part IIIVictor ChanОценок пока нет
- Upper GI Cancer MDT Approach For Med4 2017 Wo VideoДокумент34 страницыUpper GI Cancer MDT Approach For Med4 2017 Wo VideoVictor ChanОценок пока нет
- Edexcel GCE: Statistics S2Документ16 страницEdexcel GCE: Statistics S2Victor ChanОценок пока нет
- O&T - Foot and AnkleДокумент2 страницыO&T - Foot and AnkleVictor ChanОценок пока нет
- Red Cells & Whole Blood DosageДокумент4 страницыRed Cells & Whole Blood DosageVictor ChanОценок пока нет
- The FRCPath Exam - Paul BennettДокумент130 страницThe FRCPath Exam - Paul BennettVictor ChanОценок пока нет
- Initial ManagementДокумент2 страницыInitial ManagementVictor ChanОценок пока нет
- QuДокумент2 страницыQuVictor ChanОценок пока нет
- Ort 24123Документ14 страницOrt 24123Victor ChanОценок пока нет
- Chapter 2 Solutions To Practice ProblemsДокумент3 страницыChapter 2 Solutions To Practice ProblemsVictor ChanОценок пока нет
- Chapter 3 Solutions To Practice ProblemsДокумент3 страницыChapter 3 Solutions To Practice ProblemsVictor ChanОценок пока нет
- Passive VoiceДокумент2 страницыPassive VoiceVictor ChanОценок пока нет
- Voice Usage in Obama's Inaugural AddressДокумент2 страницыVoice Usage in Obama's Inaugural AddressVictor ChanОценок пока нет
- Astronomy Exam 1 Version CДокумент8 страницAstronomy Exam 1 Version CVictor ChanОценок пока нет
- Chapter 1 Solutions To Practice ProblemsДокумент3 страницыChapter 1 Solutions To Practice ProblemsVictor ChanОценок пока нет
- Astronomy 1 Exam 3 Sample: BrighterДокумент7 страницAstronomy 1 Exam 3 Sample: BrighterVictor ChanОценок пока нет
- Read Each Question Carefully, and Choose The Best AnswerДокумент7 страницRead Each Question Carefully, and Choose The Best AnswerVictor ChanОценок пока нет
- Chapter 3 Discrete Probability Distributions - Final 3Документ27 страницChapter 3 Discrete Probability Distributions - Final 3Victor ChanОценок пока нет
- A1 Exam3 SampleДокумент7 страницA1 Exam3 SampleVictor ChanОценок пока нет
- June 1012Документ16 страницJune 1012Yasir RizaОценок пока нет
- Astronomy I Exam II Sample QuestionsДокумент7 страницAstronomy I Exam II Sample QuestionsVictor ChanОценок пока нет
- 6BI08 01 Que 20130114Документ20 страниц6BI08 01 Que 20130114Islam ElsayedОценок пока нет
- 6bi08 6B Biology Jan 2011 PaperДокумент16 страниц6bi08 6B Biology Jan 2011 PaperzinmОценок пока нет
- Passive VoiceДокумент2 страницыPassive VoiceVictor ChanОценок пока нет
- 6BI08 01 Que 20120307Документ16 страниц6BI08 01 Que 20120307Fatima SaqiОценок пока нет
- 6BI08 June 2011Документ16 страниц6BI08 June 2011areyouthere92Оценок пока нет
- Construction Safety Plan GuideДокумент13 страницConstruction Safety Plan Guideemmanueloboh92% (25)
- Atr 72-500 Pilot HandbookДокумент27 страницAtr 72-500 Pilot HandbookFredyRedDevilz88% (8)
- Aiesl Sms Manual Issue II Rev 0Документ99 страницAiesl Sms Manual Issue II Rev 0Ashmi Shaji100% (1)
- 48 Safety Aspects of Industrial DryersДокумент29 страниц48 Safety Aspects of Industrial DryersVama DevОценок пока нет
- Chapter #03 MotionДокумент27 страницChapter #03 MotionSIR USMAN KHAN100% (5)
- DynamicsSlides PDFДокумент39 страницDynamicsSlides PDFSalman HussainОценок пока нет
- Operation and Maintenance Manual for Telescopic LiftsДокумент0 страницOperation and Maintenance Manual for Telescopic LiftsJose Gabriel Almonacid Gonzalez80% (5)
- Answer Sheet - The Daily Test - Group 4Документ3 страницыAnswer Sheet - The Daily Test - Group 4Hasan PerfumeОценок пока нет
- Accident ProcedureДокумент10 страницAccident ProcedureJavaid SalimОценок пока нет
- Battlecars RulebookДокумент16 страницBattlecars RulebookCarl Dettlinger50% (2)
- Supplementary Notes - Chapter 4 - Lattice VibrationДокумент43 страницыSupplementary Notes - Chapter 4 - Lattice VibrationsurendergunalanОценок пока нет
- Sample Question On Contract LawДокумент6 страницSample Question On Contract LawNik Nur Fatehah50% (2)
- Cabin Crew Duties 300 Service SafetyДокумент3 страницыCabin Crew Duties 300 Service SafetyElena OjedaОценок пока нет
- The Main Factors That Cause Car AccidentДокумент3 страницыThe Main Factors That Cause Car AccidentIvanОценок пока нет
- Emergency Response Plan Flowchart AppendixДокумент1 страницаEmergency Response Plan Flowchart Appendixe cubeОценок пока нет
- SafetySpeak! Vol 9 No 2Документ6 страницSafetySpeak! Vol 9 No 2Shikhin GargОценок пока нет
- Saratov Airlines Flight 703Документ5 страницSaratov Airlines Flight 703Yair FernanОценок пока нет
- PN eGCA (July2020)Документ2 страницыPN eGCA (July2020)DosОценок пока нет
- Scenario A320 Unprepared Emergency Crash LandingДокумент2 страницыScenario A320 Unprepared Emergency Crash Landingme2 koreancosmeticОценок пока нет
- Vda de Imperial V Heald Lumber CompanyДокумент4 страницыVda de Imperial V Heald Lumber CompanyMaria Jennifer Yumul BorbonОценок пока нет
- Types of Insurance PowerPoint 1.10.1.G1Документ30 страницTypes of Insurance PowerPoint 1.10.1.G1alizainwarraichОценок пока нет
- Dossier Ingles PDFДокумент73 страницыDossier Ingles PDFcristinacruuzОценок пока нет
- Accident FRQДокумент2 страницыAccident FRQapi-240158555Оценок пока нет
- IVC Enables Vehicle Safety and CommunicationДокумент41 страницаIVC Enables Vehicle Safety and CommunicationMahaManthra40% (5)
- The Ideal School Lunch: Traffic Wrecks Soar On Hwy. 17Документ32 страницыThe Ideal School Lunch: Traffic Wrecks Soar On Hwy. 17BayAreaNewsGroupОценок пока нет
- HIRARC Risk AssessmentДокумент1 страницаHIRARC Risk AssessmentRobiyyana100% (3)
- Rail Safety CanadaДокумент26 страницRail Safety CanadaBruno ThiemeОценок пока нет
- PN A320neo EngineДокумент3 страницыPN A320neo Enginebhartisingh0812Оценок пока нет
- Domino TheoryДокумент8 страницDomino TheorysadiaОценок пока нет
- Savarkar Short Story: Savvy SavarkarДокумент3 страницыSavarkar Short Story: Savvy SavarkarAnurupa CinarОценок пока нет