Вам также может понравиться
- Oxygen TherapyДокумент2 страницыOxygen TherapyPhilip MusonyeОценок пока нет
- Targeting Oxygen Saturation in the NICUДокумент6 страницTargeting Oxygen Saturation in the NICUaseelОценок пока нет
- COVID-19 Guidelines for Management of PatientsДокумент2 страницыCOVID-19 Guidelines for Management of PatientsSpecial OPD SVMCHRCОценок пока нет
- Niv HFNCДокумент15 страницNiv HFNCFrank VaronaОценок пока нет
- Oxygen AdminДокумент4 страницыOxygen AdminMonica SurduОценок пока нет
- NCP - Or-Rotation 2Документ12 страницNCP - Or-Rotation 2Vian RiveraОценок пока нет
- TreatmentProtocol 10-4-2021Документ3 страницыTreatmentProtocol 10-4-2021Anishk SinghОценок пока нет
- Medical Interventions for NewbornsДокумент3 страницыMedical Interventions for NewbornsCorinneОценок пока нет
- Terapi Oxygen Pada Pasien Covd-19Документ24 страницыTerapi Oxygen Pada Pasien Covd-19normamОценок пока нет
- Nursing Care Plan Cues Nursing Diagnosis Objectives Intervention Rationale EvaluationДокумент10 страницNursing Care Plan Cues Nursing Diagnosis Objectives Intervention Rationale EvaluationMargareth GonzalesОценок пока нет
- Peds 2 - Pulmonary Disorders of ChildrenДокумент27 страницPeds 2 - Pulmonary Disorders of ChildrenMinh Nguyễn Phương HồngОценок пока нет
- DR Anu Sachdeva Rational Use of Oxygen in NeonatesДокумент11 страницDR Anu Sachdeva Rational Use of Oxygen in NeonatesBhoomika PandeyОценок пока нет
- Oxygen Therapy Guide for COVID PatientsДокумент44 страницыOxygen Therapy Guide for COVID PatientsISHITA VYASОценок пока нет
- Dr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, KolkataДокумент19 страницDr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, Kolkatacy_alcantaraОценок пока нет
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG: STGДокумент4 страницыAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG: STGLiana Louisse JoseОценок пока нет
- Sari Clinical Care Training Learning Sequence 6 Oxygen TherapyДокумент22 страницыSari Clinical Care Training Learning Sequence 6 Oxygen TherapyEstefania Cuta HernandezОценок пока нет
- CPG BronchiolitisДокумент4 страницыCPG BronchiolitisLouis SudarioОценок пока нет
- Home Oxygen For COVID 19 Patients76 1Документ1 страницаHome Oxygen For COVID 19 Patients76 1Nancy LОценок пока нет
- DR Lodha Oxygen Therapy in Covid-19 PedsДокумент30 страницDR Lodha Oxygen Therapy in Covid-19 PedsBhoomika PandeyОценок пока нет
- Assessment Nursing Diagnosis Goal of Care Outcome Criteria Interventions and Rationale EvaluationДокумент2 страницыAssessment Nursing Diagnosis Goal of Care Outcome Criteria Interventions and Rationale EvaluationMariah Angela PonceОценок пока нет
- Postanesthesia Care Recovery Phases Equipment StaffingДокумент36 страницPostanesthesia Care Recovery Phases Equipment StaffingAbu Bakr Ar RaziОценок пока нет
- BRONCHOPULMONARY DYSPLASIA ModifiedДокумент48 страницBRONCHOPULMONARY DYSPLASIA ModifiedajanmjОценок пока нет
- Materi WS NIV ANU 2022 - High Flow Nasal Cannula (HFNC)Документ32 страницыMateri WS NIV ANU 2022 - High Flow Nasal Cannula (HFNC)dyahОценок пока нет
- NCP For OxygenationДокумент6 страницNCP For OxygenationChriz LechОценок пока нет
- Pediatrics-Respiratory Disorders of The Newborn: Diseases Clinical Manifestations Diagnosis & Prognosis ManagementДокумент9 страницPediatrics-Respiratory Disorders of The Newborn: Diseases Clinical Manifestations Diagnosis & Prognosis ManagementJonathan ZumakpehОценок пока нет
- utsaДокумент17 страницutsaCallie ParkОценок пока нет
- Respiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelineДокумент32 страницыRespiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelinePediatri UnsratОценок пока нет
- GINA AlgorithmДокумент6 страницGINA AlgorithmMarcela YolinaОценок пока нет
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationДокумент3 страницыAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationAlyОценок пока нет
- European Consensus On The Management of RDSДокумент41 страницаEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- HFNC Guidelines AustraliaДокумент13 страницHFNC Guidelines AustraliaMASIEL AMELIA BARRANTES ARCEОценок пока нет
- Guidance on Oxygen Therapy for COVID-19 PatientsДокумент1 страницаGuidance on Oxygen Therapy for COVID-19 PatientsAsh mohamedОценок пока нет
- Pharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptДокумент27 страницPharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptLeni Fitriani HamduОценок пока нет
- Child - Bronchiolitis NCPДокумент2 страницыChild - Bronchiolitis NCPjoeti80% (5)
- Surfactant Use in Resuscitation: Dr. Adhi, Sp.A (K)Документ21 страницаSurfactant Use in Resuscitation: Dr. Adhi, Sp.A (K)Mahyarani DalimuntheОценок пока нет
- Case 4Документ11 страницCase 4Shakshi RainaОценок пока нет
- Surfactant Replacement Therapy - 2019Документ8 страницSurfactant Replacement Therapy - 2019Saravanan Nallasivan100% (2)
- HFNC FinalДокумент42 страницыHFNC FinalAbhilasha Singh PanwarОценок пока нет
- Administering Oxygen by Nasal CannulaДокумент5 страницAdministering Oxygen by Nasal CannulaAndrea Bayaga WaganОценок пока нет
- Status AsthmaticusДокумент6 страницStatus AsthmaticusMae Azores100% (1)
- NCP For Nuchal CordДокумент6 страницNCP For Nuchal CordAubrey Marie GuerreroОценок пока нет
- High Flow Nasal Canula: Management of COVID-19 Patients: Department of Nursing Education and ResearchДокумент12 страницHigh Flow Nasal Canula: Management of COVID-19 Patients: Department of Nursing Education and ResearchIfan SetiadiОценок пока нет
- Ncma 219 Rle ReviewerДокумент7 страницNcma 219 Rle ReviewerAngelica AdlawanОценок пока нет
- NIV ProformaДокумент10 страницNIV ProformaWael N Sh GadallaОценок пока нет
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationДокумент10 страницAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaОценок пока нет
- Local Anaesthetics: Essential Guide to Properties and MechanismsДокумент17 страницLocal Anaesthetics: Essential Guide to Properties and MechanismsaliОценок пока нет
- 7 - Oxygen &exchangeДокумент16 страниц7 - Oxygen &exchange.Оценок пока нет
- Terapi Oksigen PDFДокумент50 страницTerapi Oksigen PDFelianamuis100% (1)
- Nursing Care Plan 6 Impaired Gas ExchangeДокумент9 страницNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- 01 - Bronchial AsthmaДокумент6 страниц01 - Bronchial AsthmaFrank VaronaОценок пока нет
- High-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningДокумент3 страницыHigh-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningMahmoud khedrОценок пока нет
- Tachypnoea Predicts Hypoxia in Acutely Ill InfantsДокумент4 страницыTachypnoea Predicts Hypoxia in Acutely Ill Infantsmuthia khairunnisaОценок пока нет
- Management of COVID-19 in ChildrenДокумент10 страницManagement of COVID-19 in ChildrenJuhi NeogiОценок пока нет
- Rita Care PlanДокумент2 страницыRita Care Planapi-398600648100% (1)
- Trust Guideline For Neonatal Volume Guarantee Ventilation (VGV)Документ8 страницTrust Guideline For Neonatal Volume Guarantee Ventilation (VGV)mohamedkorieshОценок пока нет
- RDS Case Study: Preterm Infant with Respiratory DistressДокумент4 страницыRDS Case Study: Preterm Infant with Respiratory DistressE.R.OОценок пока нет
- A Guide To Early Treatment of COVID-19: First Line TherapiesДокумент4 страницыA Guide To Early Treatment of COVID-19: First Line TherapiesHector CorralesОценок пока нет
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingОт EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingОценок пока нет
- Jurnal Luka SetrumДокумент4 страницыJurnal Luka Setrumuchii02Оценок пока нет
- Diagnosis THT (ICD)Документ2 страницыDiagnosis THT (ICD)uchii02100% (1)
- Daftar PustakaДокумент1 страницаDaftar Pustakauchii02Оценок пока нет
- Gender Dif in Panic DisДокумент4 страницыGender Dif in Panic Disuchii02Оценок пока нет
- Tugas Kelompok Potential Space of Head and NeckДокумент7 страницTugas Kelompok Potential Space of Head and Neckuchii02Оценок пока нет
- Are Antipsychotics OverprescribedДокумент7 страницAre Antipsychotics Overprescribeduchii02Оценок пока нет
- Pulse Icd 10 eДокумент16 страницPulse Icd 10 euchii02Оценок пока нет
- Malpractice: Your Informed Consent May Not Be Good Enough: Lee J. Johnson, JD Posted: 02/10/2011Документ3 страницыMalpractice: Your Informed Consent May Not Be Good Enough: Lee J. Johnson, JD Posted: 02/10/2011uchii02Оценок пока нет
- Lepas Alas KakiДокумент1 страницаLepas Alas Kakiuchii02Оценок пока нет
- Case Report Blok Elektif YarsiДокумент11 страницCase Report Blok Elektif Yarsiuchii02Оценок пока нет
- Allergic RhinitisДокумент12 страницAllergic Rhinitisuchii02Оценок пока нет
- Critical Therapy Study ResultsДокумент4 страницыCritical Therapy Study ResultsAinur 'iin' RahmahОценок пока нет
- Clostridium Difficile Infection Fidaxomicin Esnm1Документ11 страницClostridium Difficile Infection Fidaxomicin Esnm1Pet UrОценок пока нет
- Mental RetardationДокумент34 страницыMental RetardationJhon Cristian M. TolentinoОценок пока нет
- Glutathione and Its Antiaging and Antimelanogenic EffectsДокумент7 страницGlutathione and Its Antiaging and Antimelanogenic EffectsG. I.Оценок пока нет
- Revista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticoДокумент13 страницRevista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticocysagasОценок пока нет
- YOGA THERAPY for Digestive HealthДокумент3 страницыYOGA THERAPY for Digestive Healthrabirm77Оценок пока нет
- Ghid STEMI PDFДокумент66 страницGhid STEMI PDFAlina NОценок пока нет
- The Ommaya ReservoirДокумент3 страницыThe Ommaya Reservoirmnk1001Оценок пока нет
- Anal FissuresДокумент2 страницыAnal FissureskhadzxОценок пока нет
- On Being Alone: Guide For Widowed PersonsДокумент12 страницOn Being Alone: Guide For Widowed PersonsWinterSpringОценок пока нет
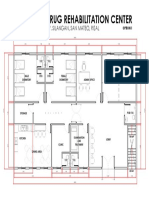
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalДокумент1 страницаProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonОценок пока нет
- A Seminar Report On "Attitude": Seth Jai Parkash Mukand Lal Institute of Engineering and Technology, Radaur (Yamunanagar)Документ20 страницA Seminar Report On "Attitude": Seth Jai Parkash Mukand Lal Institute of Engineering and Technology, Radaur (Yamunanagar)BamanОценок пока нет
- Hook Nail Deformity Surgical Treatment With A Homodigital Advancement Flap 1995 The Journal of Hand Surgery British European VolumeДокумент6 страницHook Nail Deformity Surgical Treatment With A Homodigital Advancement Flap 1995 The Journal of Hand Surgery British European VolumeProfesseur Christian DumontierОценок пока нет
- AnemiaДокумент40 страницAnemiaRajaОценок пока нет
- Illness BehaviorДокумент11 страницIllness BehaviorRubelleMicahCagampangSapongОценок пока нет
- SMLE 2019 CorrectionsДокумент112 страницSMLE 2019 CorrectionsRight VentricleОценок пока нет
- 14 03-21 Cord CareДокумент16 страниц14 03-21 Cord Careapi-250478881Оценок пока нет
- FOLIE A DEUX REVIEWДокумент8 страницFOLIE A DEUX REVIEWGrandfather NurgleОценок пока нет
- Yashica PDFДокумент7 страницYashica PDFmindpriestsОценок пока нет
- Emergency Medical Technician CPGs PDFДокумент121 страницаEmergency Medical Technician CPGs PDFAnonymous OdW7ev100% (1)
- NeuroblastomaДокумент10 страницNeuroblastomadita100% (1)
- EnglishДокумент56 страницEnglishPankaj SharmaОценок пока нет
- Chapter 1 - Psychology As A ScienceДокумент21 страницаChapter 1 - Psychology As A Sciencevarunas_250% (2)
- Overview of Skin Aging and PhotoagingДокумент7 страницOverview of Skin Aging and PhotoagingtissanОценок пока нет
- Unit 2 - TYPES OF RECREATION Part 2Документ22 страницыUnit 2 - TYPES OF RECREATION Part 2Reina100% (6)
- Child Psychiatric DisordersДокумент8 страницChild Psychiatric DisordersGaurang ShirwadkarОценок пока нет
- NCP - Acute Pain Stomach CancerДокумент2 страницыNCP - Acute Pain Stomach CancerJohn Michael TaylanОценок пока нет
- Reumatoid ArthritisДокумент19 страницReumatoid Arthritishenning_mastereid166Оценок пока нет
- Trigger Finger PostopДокумент2 страницыTrigger Finger PostopNandaSuryaWijayaОценок пока нет
- Competences Required For Effective Systemic TherapiesДокумент27 страницCompetences Required For Effective Systemic TherapiesJosé BernalОценок пока нет
- Rechilding Creating A New Past in The Present As A Support For The FutureДокумент10 страницRechilding Creating A New Past in The Present As A Support For The FutureBojanaОценок пока нет