Вам также может понравиться
- Pi Is 0168827817319955Документ3 страницыPi Is 0168827817319955kookyinОценок пока нет
- HBV Therapy - Slide DeckДокумент28 страницHBV Therapy - Slide DeckUddalak ChakrabortyОценок пока нет
- Ingeniería Genética I: Transferencia HorizontalДокумент12 страницIngeniería Genética I: Transferencia HorizontalHandball AmeliaОценок пока нет
- Molec Gen PanДокумент14 страницMolec Gen PanPannathorn SiriОценок пока нет
- Immunology MaterialДокумент12 страницImmunology MaterialFatimah RizkyОценок пока нет
- Snapshot Cancer Immunotherapy 1681565886Документ2 страницыSnapshot Cancer Immunotherapy 1681565886samanehr1Оценок пока нет
- Review: Predicted Immune ResponsesДокумент2 страницыReview: Predicted Immune ResponsesAntonio de Jesús Garcia A.Оценок пока нет
- Exinator2: Whole Genome Somatic MutationsДокумент1 страницаExinator2: Whole Genome Somatic MutationsshoummowОценок пока нет
- Chronic Hepatitis B NEJM 2022Документ15 страницChronic Hepatitis B NEJM 2022Πάνος ΣταγήςОценок пока нет
- Hepatitis BДокумент6 страницHepatitis BCarmen MargoОценок пока нет
- SARS-CoV-2 Variants - UK + South African + Brazil Variants - Key AtfДокумент1 страницаSARS-CoV-2 Variants - UK + South African + Brazil Variants - Key AtfJuan Manuel Tapia AlzateОценок пока нет
- 1 s2.0 S0168827809003894 Main PDFДокумент12 страниц1 s2.0 S0168827809003894 Main PDFAbdullah M AbdullahОценок пока нет
- Molecular Biology Workflow Solutions BrochureДокумент56 страницMolecular Biology Workflow Solutions BrochureBishoy F. YoussefОценок пока нет
- Molecular Biology Workflow Solutions BrochureДокумент62 страницыMolecular Biology Workflow Solutions BrochureJoséMaríaMoralesMuñozОценок пока нет
- EUKARYOTIC DNA VIRUSES - Temporal Control: 1. Simian Virus 40Документ2 страницыEUKARYOTIC DNA VIRUSES - Temporal Control: 1. Simian Virus 40Maria August P. PrudencioОценок пока нет
- Transcription FactorsДокумент13 страницTranscription Factorsfazila zahoorОценок пока нет
- The Scientist - Winter 2023Документ92 страницыThe Scientist - Winter 2023Martha LopushynskaОценок пока нет
- RNa Pol & PromotersДокумент12 страницRNa Pol & Promotersfazila zahoorОценок пока нет
- III. Gen Perk S2 - DIR 2021 - Pengontrolan Ekspresi GenДокумент17 страницIII. Gen Perk S2 - DIR 2021 - Pengontrolan Ekspresi GenSisy YuliantyОценок пока нет
- The Complement Cascade: Membrane Attack ComplexДокумент2 страницыThe Complement Cascade: Membrane Attack ComplexGibran Meza CastrejonОценок пока нет
- Multi Scenes Usage Fluorescence Immunoassay Analyzer: SpecificationДокумент2 страницыMulti Scenes Usage Fluorescence Immunoassay Analyzer: Specificationdanang setiawanОценок пока нет
- 8 Inheritance and EvolutionДокумент1 страница8 Inheritance and EvolutionMeiying LeeОценок пока нет
- Overview - Regulation of ApoptosisДокумент1 страницаOverview - Regulation of ApoptosisAym mantezОценок пока нет
- Catatan ITP Dan AAДокумент17 страницCatatan ITP Dan AAngurahardhi88Оценок пока нет
- NullДокумент1 страницаNullapi-16525854Оценок пока нет
- Folwchart NGSДокумент3 страницыFolwchart NGSกรวรินทร์ ชำนาญกุลОценок пока нет
- Lab DiagnosisДокумент4 страницыLab DiagnosisKushalaniОценок пока нет
- Hepatitis B Virus Replication: Series EditorДокумент17 страницHepatitis B Virus Replication: Series EditorMarius StancuОценок пока нет
- RBC & It's DisorderДокумент101 страницаRBC & It's DisorderSОценок пока нет
- T Cell Receptor Signaling: F-A CtinДокумент2 страницыT Cell Receptor Signaling: F-A CtinOlgaОценок пока нет
- Hepatitis B Virus: Trends in MicrobiologyДокумент2 страницыHepatitis B Virus: Trends in MicrobiologyDyna Ratnasari PlashintaniaОценок пока нет
- 1 - UK Lamuno Plus BrochureДокумент2 страницы1 - UK Lamuno Plus BrochurePhyo WaiОценок пока нет
- Psoriasis and Cardiovascular Disease: Where Is The Risk?: CommentaryДокумент4 страницыPsoriasis and Cardiovascular Disease: Where Is The Risk?: CommentarySaifuddin HaswareОценок пока нет
- Poster Complet v2Документ1 страницаPoster Complet v2SANVITTAYAGUL PronsagornОценок пока нет
- Elimination of Infectious HIV DNA by CRISPR-Cas9: Atze T Das, Caroline S Binda and Ben BerkhoutДокумент8 страницElimination of Infectious HIV DNA by CRISPR-Cas9: Atze T Das, Caroline S Binda and Ben BerkhoutMônica MoreliОценок пока нет
- Review: Treatment With Repurposed DrugsДокумент5 страницReview: Treatment With Repurposed DrugsmwdhtirahОценок пока нет
- Hematology Pathology - 003) Acute Lymphoblastic Leukemia (ALL) (Illustrations - Key)Документ1 страницаHematology Pathology - 003) Acute Lymphoblastic Leukemia (ALL) (Illustrations - Key)hasanatiya41Оценок пока нет
- BiomoleculesДокумент12 страницBiomoleculesPRADEEP CОценок пока нет
- Dna Rna Protein: To Make New Copy of DNA Occurs Before Cell Division Important For Tissue Repair and GrowthДокумент1 страницаDna Rna Protein: To Make New Copy of DNA Occurs Before Cell Division Important For Tissue Repair and GrowthKho Swee LiangОценок пока нет
- Classification of AnaemiaДокумент1 страницаClassification of Anaemianmyza89Оценок пока нет
- Janeway's Immunobiology 8thДокумент892 страницыJaneway's Immunobiology 8thSergio Falcon Rivera92% (12)
- USFDA Approved PKIsДокумент19 страницUSFDA Approved PKIsAnamaria IuoraşОценок пока нет
- CRISPR InfographicДокумент1 страницаCRISPR InfographicSantino Dev Joseph Xavier (Sji)Оценок пока нет
- 3.5 NotesДокумент14 страниц3.5 Noteslaeticia schmiesОценок пока нет
- HP F10 Presentation Genome EditingДокумент21 страницаHP F10 Presentation Genome EditingToros TaşgınОценок пока нет
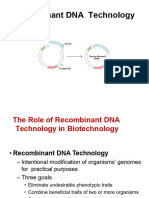
- Recombinant DNA Technology 2023Документ29 страницRecombinant DNA Technology 2023Ana Laura Mendoza AriasОценок пока нет
- ViruzhinkiДокумент20 страницViruzhinkiЕгор ЧудовскийОценок пока нет
- An Overview of Candidate Immunologic Biomarkers and Surrogate MarkersДокумент31 страницаAn Overview of Candidate Immunologic Biomarkers and Surrogate Markersantonio pОценок пока нет
- Transcription )Документ5 страницTranscription )Kotchaphan ChansawangОценок пока нет
- Amyloid Plaque and Neurofibrillary Tangle Formation in Alzheimer's DiseaseДокумент2 страницыAmyloid Plaque and Neurofibrillary Tangle Formation in Alzheimer's DiseaseMelanieОценок пока нет
- Bacterial Strains For Protein ExpressionДокумент6 страницBacterial Strains For Protein ExpressionJaya SaputraОценок пока нет
- Início Da TranscriçãoДокумент10 страницInício Da TranscriçãoEmilyОценок пока нет
- RT PCR Gene Expression Intro v8Документ1 страницаRT PCR Gene Expression Intro v8ChristineDanОценок пока нет
- PHLEBOTOMYДокумент21 страницаPHLEBOTOMYmyka brilliant cristobalОценок пока нет
- Https - Learn - Cellsignal.com - Hubfs - Pdfs - 15 Fly Alzh Ref m096 Eng 00 Alzheimers PW Handout DigitalДокумент2 страницыHttps - Learn - Cellsignal.com - Hubfs - Pdfs - 15 Fly Alzh Ref m096 Eng 00 Alzheimers PW Handout DigitaltamaraОценок пока нет
- Image YyДокумент3 страницыImage YyjoudОценок пока нет
- Lecture 4 - Transcription and Post Transcription ModificationsДокумент73 страницыLecture 4 - Transcription and Post Transcription ModificationskibzwanjikuОценок пока нет
- Gateway Technology: R-DNA Technology M.Phil. Biotechnology 1st Semester CBM, University of SwatДокумент13 страницGateway Technology: R-DNA Technology M.Phil. Biotechnology 1st Semester CBM, University of SwatGul AfshaОценок пока нет
- Maglumi 600Документ4 страницыMaglumi 600DwitaRiadiniОценок пока нет
- Use of Microscope PDFДокумент7 страницUse of Microscope PDFDdn RmaОценок пока нет
- Paper Subtitle As Needed: Math in Paper Title or Abstract. The Abstract Should Be Between 150-250 WordsДокумент1 страницаPaper Subtitle As Needed: Math in Paper Title or Abstract. The Abstract Should Be Between 150-250 WordsDdn RmaОценок пока нет
- Garcinia Kola ThesisДокумент36 страницGarcinia Kola ThesisDdn RmaОценок пока нет
- Bacteremia Due To Bacteroides Fragilis Group: Distribution of Species, - Lactamase Production, and Antimicrobial Susceptibility PatternsДокумент6 страницBacteremia Due To Bacteroides Fragilis Group: Distribution of Species, - Lactamase Production, and Antimicrobial Susceptibility PatternsDdn RmaОценок пока нет
- Makalah SleДокумент48 страницMakalah Slesalini_sadhna17Оценок пока нет
- How Microorganism Cause DiseaseДокумент16 страницHow Microorganism Cause DiseaseMARTINEZ JUSTINEОценок пока нет
- Lymphatic System TransДокумент17 страницLymphatic System TransRheeanne AmilasanОценок пока нет
- Chronic Hepatitis BДокумент5 страницChronic Hepatitis BMurat HessesОценок пока нет
- The Ten Best Tools To Boost Your Immune SystemДокумент347 страницThe Ten Best Tools To Boost Your Immune SystemmamedeiaОценок пока нет
- PsiconeuroinmunologíaДокумент10 страницPsiconeuroinmunologíaLuis Alfredo Rosales GuerreroОценок пока нет
- Immune Dysfunction and Risk of Infection in CKD - 2019Документ8 страницImmune Dysfunction and Risk of Infection in CKD - 2019Lú VillalobosОценок пока нет
- Lecture - Week 3 (Natural Immunity & Complement System)Документ5 страницLecture - Week 3 (Natural Immunity & Complement System)rennel ybarolaОценок пока нет
- Virology MCQДокумент62 страницыVirology MCQGazi Shahinur Akter ShampaОценок пока нет
- Broad Spectrum Antiviral Properties of AndrographolideДокумент16 страницBroad Spectrum Antiviral Properties of Andrographolide2730810Оценок пока нет
- AACC 10 AbstractBook PDFДокумент276 страницAACC 10 AbstractBook PDFmsnsaikiranОценок пока нет
- Covid 19Документ22 страницыCovid 19imad khanОценок пока нет
- ImmunoSerology - Review Questions (Stevens)Документ14 страницImmunoSerology - Review Questions (Stevens)LUALHATI VILLAS0% (1)
- Infecciones Virales Del SNCДокумент246 страницInfecciones Virales Del SNCpediatria hncase100% (1)
- Annual Report 2019 2020Документ248 страницAnnual Report 2019 2020Prince PanwarОценок пока нет
- Immunopharmacological Perspective On Zinc in SARS-CoV-2 InfectionДокумент16 страницImmunopharmacological Perspective On Zinc in SARS-CoV-2 InfectionW CnОценок пока нет
- Plagiarism - Report SachinДокумент46 страницPlagiarism - Report SachinTahir HussainОценок пока нет
- BT102 - Microbiology (Solved Questions FINAL TERM (PAST PAPERS)Документ33 страницыBT102 - Microbiology (Solved Questions FINAL TERM (PAST PAPERS)Awais BhuttaОценок пока нет
- Dr. Trifena - PRESENTASI ESPRO-Application of Ozone Therapy For Holistic Wellness and AntiagingДокумент34 страницыDr. Trifena - PRESENTASI ESPRO-Application of Ozone Therapy For Holistic Wellness and AntiagingAdi Sutriwanto PasaribuОценок пока нет
- ISBBhandoutДокумент55 страницISBBhandoutRed GillianОценок пока нет
- Pharma ExamДокумент7 страницPharma ExamGeno Adrian T PampangaОценок пока нет
- The Use of Phyllanthus Niruri L As An ImmunomodulaДокумент10 страницThe Use of Phyllanthus Niruri L As An ImmunomodulaMuhammad Arif MahfudinОценок пока нет
- Bob Beck Protocol - Natural Cancer Treatments at CancerTutorДокумент4 страницыBob Beck Protocol - Natural Cancer Treatments at CancerTutorThiago NunesОценок пока нет
- Q1. What Is Vaccine?: Vaccinology Lecture NotesДокумент31 страницаQ1. What Is Vaccine?: Vaccinology Lecture Notesحوراء موجد هادي غاويОценок пока нет
- Kuby Immunology 7e TBДокумент134 страницыKuby Immunology 7e TBStarrx71494% (18)
- Interferon AlphaДокумент22 страницыInterferon AlphaFedri BaysarОценок пока нет
- Cells: Hepatitis C Virus Infection: Host-Virus Interaction and Mechanisms of Viral PersistenceДокумент27 страницCells: Hepatitis C Virus Infection: Host-Virus Interaction and Mechanisms of Viral Persistencemuhamad deniansyahОценок пока нет
- Inflammation and HealingДокумент30 страницInflammation and HealingKoustubh JoshiОценок пока нет
- Immune Responses To Influenza VirusДокумент12 страницImmune Responses To Influenza Virusdavid onyangoОценок пока нет
- Possible Treatment and Strategies For COVID-19: Review and AssessmentДокумент16 страницPossible Treatment and Strategies For COVID-19: Review and AssessmentAni RahayuОценок пока нет