Вам также может понравиться
- GuidlineДокумент144 страницыGuidlineAbd Halim Gazali HОценок пока нет
- Herpes Simplex Virus 2 Meningitis: A Retrospective Cohort StudyДокумент7 страницHerpes Simplex Virus 2 Meningitis: A Retrospective Cohort StudyAbd Halim Gazali HОценок пока нет
- Squamous Cell Carcinoma PDFДокумент6 страницSquamous Cell Carcinoma PDFAbd Halim Gazali HОценок пока нет
- Fluroquinolon ResistenДокумент4 страницыFluroquinolon ResistenAbd Halim Gazali HОценок пока нет
- Mediator of CopdДокумент34 страницыMediator of CopdAbd Halim Gazali HОценок пока нет
- Efikasi Gadobutarol Untuk Mri KontrasДокумент10 страницEfikasi Gadobutarol Untuk Mri KontrasAbd Halim Gazali HОценок пока нет
- Treatmment 2Документ15 страницTreatmment 2Abd Halim Gazali HОценок пока нет
- Di¡erential Adaptation of Microbial Pathogens To Airways of Patients With Cystic Brosis and Chronic Obstructive Pulmonary DiseaseДокумент24 страницыDi¡erential Adaptation of Microbial Pathogens To Airways of Patients With Cystic Brosis and Chronic Obstructive Pulmonary DiseaseAbd Halim Gazali HОценок пока нет
- Comparison AntioticДокумент10 страницComparison AntioticAbd Halim Gazali HОценок пока нет
- Sekresi Tipe 3Документ13 страницSekresi Tipe 3Abd Halim Gazali HОценок пока нет
- GOLD Pocket 2016 PDFДокумент32 страницыGOLD Pocket 2016 PDFSyuhada PinemОценок пока нет
- Pyocyanin FacilitatesДокумент12 страницPyocyanin FacilitatesAbd Halim Gazali HОценок пока нет
- Antibiotik ManajemenДокумент11 страницAntibiotik ManajemenAbd Halim Gazali HОценок пока нет
- Impaired MacrophageДокумент8 страницImpaired MacrophageAbd Halim Gazali HОценок пока нет
- Pyocyanin FacilitatesДокумент12 страницPyocyanin FacilitatesAbd Halim Gazali HОценок пока нет
- Pulmonary AspergillusДокумент9 страницPulmonary AspergillusAbd Halim Gazali HОценок пока нет
- Innate Immune MacrophageДокумент9 страницInnate Immune MacrophageAbd Halim Gazali HОценок пока нет
- GTP PDFДокумент16 страницGTP PDFAbd Halim Gazali HОценок пока нет
- Diagnosis and TreatmentДокумент9 страницDiagnosis and TreatmentAbd Halim Gazali HОценок пока нет
- Fluroquinolon ResistenДокумент4 страницыFluroquinolon ResistenAbd Halim Gazali HОценок пока нет
- Effect MrytolДокумент9 страницEffect MrytolAbd Halim Gazali HОценок пока нет
- Di¡erential Adaptation of Microbial Pathogens To Airways of Patients With Cystic Brosis and Chronic Obstructive Pulmonary DiseaseДокумент24 страницыDi¡erential Adaptation of Microbial Pathogens To Airways of Patients With Cystic Brosis and Chronic Obstructive Pulmonary DiseaseAbd Halim Gazali HОценок пока нет
- AzitromisinДокумент13 страницAzitromisinAbd Halim Gazali HОценок пока нет
- Apoptosis MakrofagДокумент11 страницApoptosis MakrofagAbd Halim Gazali HОценок пока нет
- Biofilm ResistanceДокумент9 страницBiofilm ResistanceAbd Halim Gazali HОценок пока нет
- EfwefrgДокумент13 страницEfwefrgAbd Halim Gazali HОценок пока нет
- J Neurol Neurosurg Psychiatry 2004 Kennedy I10 5Документ7 страницJ Neurol Neurosurg Psychiatry 2004 Kennedy I10 5Ronald Ivan WijayaОценок пока нет
- An ImmunologicallyДокумент10 страницAn ImmunologicallyAbd Halim Gazali HОценок пока нет
- Orrelation With RadiologicДокумент6 страницOrrelation With RadiologicAbd Halim Gazali HОценок пока нет
- Impaired MacrophageДокумент8 страницImpaired MacrophageAbd Halim Gazali HОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Handbook of Good Dairy Husbandry PracticesДокумент12 страницHandbook of Good Dairy Husbandry PracticesAnil JindalОценок пока нет
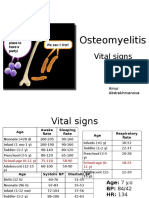
- PBL 2 - OsteomyelitisДокумент10 страницPBL 2 - OsteomyelitisAinur AbdrakhmanovaОценок пока нет
- Buffalo Public Schools ResumeДокумент1 страницаBuffalo Public Schools ResumeAdam PenaleОценок пока нет
- Fever With Rash in Table Form.Документ4 страницыFever With Rash in Table Form.Azizan HannyОценок пока нет
- State Wise Quarantine Regulations Updated As On: 03 March 2022Документ24 страницыState Wise Quarantine Regulations Updated As On: 03 March 2022Ashutosh MaiidОценок пока нет
- Aquifer Case - Summary - FamilyMedicine23 - 5-YeДокумент9 страницAquifer Case - Summary - FamilyMedicine23 - 5-YeHyunsoo EllisОценок пока нет
- Daftar Pustaka: Raka, L, 2010Документ2 страницыDaftar Pustaka: Raka, L, 2010dnoksОценок пока нет
- Noushad RT-PCR TEST REPORT 2Документ2 страницыNoushad RT-PCR TEST REPORT 2kabirОценок пока нет
- Malaria Symptoms and CausesДокумент12 страницMalaria Symptoms and CausesWidia YuniОценок пока нет
- Tuberculous MeningitisДокумент8 страницTuberculous MeningitisEchizen RukawaОценок пока нет
- Pediatric ExamДокумент11 страницPediatric ExamRamones JokerОценок пока нет
- Quize EpiДокумент38 страницQuize EpiAbdulla AldoseriОценок пока нет
- Laboratory Response Checklist For Infectious Disease Outbreaks-Preparedness and Response Considerations For Emerging ThreatsДокумент11 страницLaboratory Response Checklist For Infectious Disease Outbreaks-Preparedness and Response Considerations For Emerging ThreatsamabelОценок пока нет
- Louis Pasteur's Contributions to MicrobiologyДокумент2 страницыLouis Pasteur's Contributions to MicrobiologyAnn MalitОценок пока нет
- Entamoeba histolytica ParasiteДокумент32 страницыEntamoeba histolytica ParasiteAngela FovinaОценок пока нет
- Form A - v2017Документ2 страницыForm A - v2017Analiza ArnaldoОценок пока нет
- What Is TonsillitisДокумент4 страницыWhat Is TonsillitisAn NukmanОценок пока нет
- HPV Vaccination For All Leaflet 2020Документ8 страницHPV Vaccination For All Leaflet 2020kovi mОценок пока нет
- Full Note On MalariaДокумент23 страницыFull Note On MalariaSamuel Obeng100% (2)
- HIV and AIDS explainedДокумент1 страницаHIV and AIDS explainedKevinОценок пока нет
- STI/RTI Syndromic Case Management - NACOДокумент1 страницаSTI/RTI Syndromic Case Management - NACOTejas100% (8)
- STD Chlamydia: Causes, Symptoms, Diagnosis and TreatmentДокумент3 страницыSTD Chlamydia: Causes, Symptoms, Diagnosis and TreatmentkyawОценок пока нет
- HIV/AIDS: A Leading Cause of Death Among People Aged 25-44 Years in U.SДокумент31 страницаHIV/AIDS: A Leading Cause of Death Among People Aged 25-44 Years in U.SMuhammad Bilal Bin Amir100% (1)
- Circular No. 3 1Документ5 страницCircular No. 3 1spawnn NVX7Оценок пока нет
- Laboratory Diagnostic in Medical MycologyДокумент14 страницLaboratory Diagnostic in Medical MycologyMohamed100% (1)
- Salinan TPS 6 - Bahasa Inggris - AdeДокумент8 страницSalinan TPS 6 - Bahasa Inggris - AdeUmi Masfufah HanimОценок пока нет
- NCC (Natural Catalytic Conversion) Technology: Up To 99%Документ2 страницыNCC (Natural Catalytic Conversion) Technology: Up To 99%Neo Dinastian OnssalisОценок пока нет
- Drtbalu'S Otolaryngology Online: Acute LaryngitisДокумент3 страницыDrtbalu'S Otolaryngology Online: Acute LaryngitisAnish RajОценок пока нет
- Coronaviurs Disease - by MahiДокумент1 страницаCoronaviurs Disease - by MahiMukesh C BhartiОценок пока нет
- Dip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Документ1 страницаDip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Neo Latoya MadunaОценок пока нет