
Вам также может понравиться
- Veterinary College, Bengaluru: DR A. S. Patil, DR Ramesh Rathod, DR B. N. Nagaraj and DR L. RanganathДокумент15 страницVeterinary College, Bengaluru: DR A. S. Patil, DR Ramesh Rathod, DR B. N. Nagaraj and DR L. RanganathransinghОценок пока нет
- Veterinary College, Bengaluru: Dr. Prakash NadoorДокумент16 страницVeterinary College, Bengaluru: Dr. Prakash NadoorransinghОценок пока нет
- Fo"k LWP HДокумент50 страницFo"k LWP HransinghОценок пока нет
- Veterinary College, BengaluruДокумент20 страницVeterinary College, BengalururansinghОценок пока нет
- Fodder Box: Veterinary College, BengaluruДокумент11 страницFodder Box: Veterinary College, BengalururansinghОценок пока нет
- Feb 2015Документ16 страницFeb 2015ransinghОценок пока нет
- Veterinary College, Bengaluru: Madhukardama and Upendra H. AДокумент10 страницVeterinary College, Bengaluru: Madhukardama and Upendra H. AransinghОценок пока нет
- PPR Goat DiseaseДокумент6 страницPPR Goat DiseaseransinghОценок пока нет
- Wing RotДокумент2 страницыWing Rotransingh100% (1)
- CH 5Документ11 страницCH 5ransinghОценок пока нет
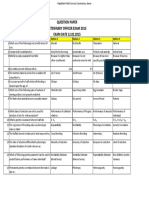
- Question Paper Veterinary Officer Exam 2013 EXAM DATE 12.02.2015Документ7 страницQuestion Paper Veterinary Officer Exam 2013 EXAM DATE 12.02.2015ransinghОценок пока нет
- Abortions in Dairy Cows PDFДокумент4 страницыAbortions in Dairy Cows PDFransinghОценок пока нет
- Early Chick MortalityДокумент2 страницыEarly Chick MortalityransinghОценок пока нет
- Jktlfkku Yksd Lsok VK KSX) VtesjДокумент1 страницаJktlfkku Yksd Lsok VK KSX) VtesjransinghОценок пока нет
- In Practice 2012 Maillard 292 9Документ9 страницIn Practice 2012 Maillard 292 9ransinghОценок пока нет
- In Practice 2012 Moores 22 6Документ6 страницIn Practice 2012 Moores 22 6ransinghОценок пока нет
- Preamble Vmo 2013 08062015Документ3 страницыPreamble Vmo 2013 08062015ransinghОценок пока нет
- Posting Orders of Sr. VO After DPC (22.12Документ10 страницPosting Orders of Sr. VO After DPC (22.12ransinghОценок пока нет
- In Practice 2012 Whitley 322 9Документ7 страницIn Practice 2012 Whitley 322 9ransinghОценок пока нет
- In Practice 2012 Moores 74 7Документ5 страницIn Practice 2012 Moores 74 7ransinghОценок пока нет
- Lec02 PDFДокумент11 страницLec02 PDFransinghОценок пока нет
- In Practice 2012 Scott 12 21Документ9 страницIn Practice 2012 Scott 12 21ransinghОценок пока нет
- In Practice 2012 Lord 156 62Документ8 страницIn Practice 2012 Lord 156 62ransinghОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Drug Study Format For RLEДокумент2 страницыDrug Study Format For RLESheryl Ann Barit PedinesОценок пока нет
- 2nd Fattahi Morphophysiological and Phytochemical Responses To Cadmium and Lead Stress in Coriander (Coriandrum Sativum L.)Документ10 страниц2nd Fattahi Morphophysiological and Phytochemical Responses To Cadmium and Lead Stress in Coriander (Coriandrum Sativum L.)Mohammad Kazem souriОценок пока нет
- PDF]Jan-Febc 2010 - Jaypee Brothers Medical Publishers jaypeebrothers.com/pdf/cataloginmonths/jan-feb2010.pdf by S Bhat - 2010 A unique book on clinical methods in surgery along with interactive DVD-ROM ... and clinical approach to each and individual surgical cases .... including a brief outline on prognosis. • Provides in-depth ..... Susmita Bhattacharya. Epidemiology. mbbs books - Scribd https://www.scribd.com/doc/239765747/mbbs-books Sep 15, 2014 - mbbs books - Download as Word Doc (.doc / .docx), PDF File (.pdf), Text ... BHATTACHARYA SHORT CASES IN SURGERY 5TH 2002 200.00 BOOKS1 - Scribd https://www.scribd.com/doc/99385577/BOOKS1 Jul 7, 2012 - BOOKS1 - Ebook download as PDF File (.pdf), Text file (.txt) or read book ... LAWRENCE W. SHORT CASES IN SURGERY / BHATTACHARYA, ... Medical Books - mbbs exam questions for second third and ... hafeesh.blogspot.com/2009/12/medical-books.html Dec 25, 2009 - GUPTE SHORT TEXTBOOK OF MEDICAL MICROBIOLOGY 8TH 2002 .... BHATTACHARYA SHORT CASESДокумент3 страницыPDF]Jan-Febc 2010 - Jaypee Brothers Medical Publishers jaypeebrothers.com/pdf/cataloginmonths/jan-feb2010.pdf by S Bhat - 2010 A unique book on clinical methods in surgery along with interactive DVD-ROM ... and clinical approach to each and individual surgical cases .... including a brief outline on prognosis. • Provides in-depth ..... Susmita Bhattacharya. Epidemiology. mbbs books - Scribd https://www.scribd.com/doc/239765747/mbbs-books Sep 15, 2014 - mbbs books - Download as Word Doc (.doc / .docx), PDF File (.pdf), Text ... BHATTACHARYA SHORT CASES IN SURGERY 5TH 2002 200.00 BOOKS1 - Scribd https://www.scribd.com/doc/99385577/BOOKS1 Jul 7, 2012 - BOOKS1 - Ebook download as PDF File (.pdf), Text file (.txt) or read book ... LAWRENCE W. SHORT CASES IN SURGERY / BHATTACHARYA, ... Medical Books - mbbs exam questions for second third and ... hafeesh.blogspot.com/2009/12/medical-books.html Dec 25, 2009 - GUPTE SHORT TEXTBOOK OF MEDICAL MICROBIOLOGY 8TH 2002 .... BHATTACHARYA SHORT CASESSaiSuryaTeja0% (1)
- Guillain-Barré SyndromeДокумент60 страницGuillain-Barré SyndromekharaОценок пока нет
- 2023 Guideline Diagnosis Management AFIB Slide SetДокумент46 страниц2023 Guideline Diagnosis Management AFIB Slide SetMARIAM BANOОценок пока нет
- Nursing Responsibilities During Radiation TherapyДокумент59 страницNursing Responsibilities During Radiation TherapyJhe Victoriano91% (22)
- Gene4PD - A Comprehensive Genetic Database of Parkinson's DiseaseДокумент11 страницGene4PD - A Comprehensive Genetic Database of Parkinson's DiseaseANCC Atma Jaya Neuroscience & Cognitive CentreОценок пока нет
- A Guide To Deep Learning in HealthcareДокумент6 страницA Guide To Deep Learning in HealthcareJeffrey SwansonОценок пока нет
- The Role of Aging and Movement Disorders: EditorsДокумент461 страницаThe Role of Aging and Movement Disorders: EditorsAntonio tapiaОценок пока нет
- Acupuncture Miriam Lee - Yin and Yang - HeartДокумент24 страницыAcupuncture Miriam Lee - Yin and Yang - HeartAurora Alina Bujor-FlueranОценок пока нет
- Module 1 Prenatal Development - PDF PDFДокумент11 страницModule 1 Prenatal Development - PDF PDFKevin PajarilloОценок пока нет
- Bio 1 C1Документ14 страницBio 1 C1selapakhiОценок пока нет
- Omsk 2Документ9 страницOmsk 2Ary Rachmat KusumaОценок пока нет
- Damps, Pamps, and Lamps in Immunity and Sterile InflammationДокумент26 страницDamps, Pamps, and Lamps in Immunity and Sterile InflammationCony G100% (1)
- Eka Bilvam & Maha Bilvam: Tissue Culture Ancient & Sacred Herbal PlantsДокумент15 страницEka Bilvam & Maha Bilvam: Tissue Culture Ancient & Sacred Herbal PlantsNavaneetha PhaniОценок пока нет
- Improving Occupational Safety Health and Risk ManagementДокумент68 страницImproving Occupational Safety Health and Risk ManagementReichstein CaduaОценок пока нет
- Nursing Care PlanДокумент3 страницыNursing Care Planjovanney100% (10)
- Thesis Dental Public HealthДокумент8 страницThesis Dental Public Healthbsem160v100% (2)
- Life Span Development 14th Edition Santrock Test Bank Full Chapter PDFДокумент57 страницLife Span Development 14th Edition Santrock Test Bank Full Chapter PDFluismackxeaiwgkbfd100% (12)
- Artis Zee EP Suite Final PDFДокумент20 страницArtis Zee EP Suite Final PDFTòng Tiêu ThanhОценок пока нет
- Asd BrochureДокумент6 страницAsd Brochureapi-504447814Оценок пока нет
- Laporan Kasus Per Gol Umur Feb 2023Документ7 страницLaporan Kasus Per Gol Umur Feb 2023Akreditasi UKPОценок пока нет
- MalariaДокумент22 страницыMalariaAbdirahmanОценок пока нет
- Case3 Case StudyДокумент6 страницCase3 Case StudyKrizzia Angela BacotocОценок пока нет
- 1.antioxidant and Functional FoodДокумент38 страниц1.antioxidant and Functional FoodnajwaОценок пока нет
- LT Marine Application TemplateДокумент4 страницыLT Marine Application TemplateEirvin JamesОценок пока нет
- Double-X Nutrition Facts PDFДокумент1 страницаDouble-X Nutrition Facts PDFS.odysseyОценок пока нет
- The Effects of Poverty On The Accessibility of Health Care in Low Income Families Within Lipa CityДокумент23 страницыThe Effects of Poverty On The Accessibility of Health Care in Low Income Families Within Lipa CityAlexa BulataoОценок пока нет
- National Voluntary Blood Services Program (Philippines)Документ2 страницыNational Voluntary Blood Services Program (Philippines)Charm Arroyo71% (7)
- Cement Retained. Vs Screw Retained Implant (Ada GuideДокумент6 страницCement Retained. Vs Screw Retained Implant (Ada GuideAsma AbdullaОценок пока нет

































































![PDF]Jan-Febc 2010 - Jaypee Brothers Medical Publishers jaypeebrothers.com/pdf/cataloginmonths/jan-feb2010.pdf by S Bhat - 2010 A unique book on clinical methods in surgery along with interactive DVD-ROM ... and clinical approach to each and individual surgical cases .... including a brief outline on prognosis. • Provides in-depth ..... Susmita Bhattacharya. Epidemiology. mbbs books - Scribd https://www.scribd.com/doc/239765747/mbbs-books Sep 15, 2014 - mbbs books - Download as Word Doc (.doc / .docx), PDF File (.pdf), Text ... BHATTACHARYA SHORT CASES IN SURGERY 5TH 2002 200.00 BOOKS1 - Scribd https://www.scribd.com/doc/99385577/BOOKS1 Jul 7, 2012 - BOOKS1 - Ebook download as PDF File (.pdf), Text file (.txt) or read book ... LAWRENCE W. SHORT CASES IN SURGERY / BHATTACHARYA, ... Medical Books - mbbs exam questions for second third and ... hafeesh.blogspot.com/2009/12/medical-books.html Dec 25, 2009 - GUPTE SHORT TEXTBOOK OF MEDICAL MICROBIOLOGY 8TH 2002 .... BHATTACHARYA SHORT CASES](https://imgv2-2-f.scribdassets.com/img/document/270707806/149x198/154b6610c1/1605034206?v=1)


























