Вам также может понравиться
- Medical Medium Thyroid Healing The TruthДокумент8 страницMedical Medium Thyroid Healing The TruthVatsala Saith0% (18)
- Inguinal HerniaДокумент25 страницInguinal HernianadiaОценок пока нет
- Morning Report: Irreponible Scrotalis HerniaДокумент36 страницMorning Report: Irreponible Scrotalis HerniaLatifah RamadaniОценок пока нет
- HERNIAДокумент70 страницHERNIAmwro789000Оценок пока нет
- 9 HerniaДокумент38 страниц9 HerniaErwin SiahaanОценок пока нет
- Hernia: RSST Klaten Koas Stase Bedah A13.1Документ54 страницыHernia: RSST Klaten Koas Stase Bedah A13.1Bagus WirayudaОценок пока нет
- Hernia RepairДокумент19 страницHernia RepairdanarfsОценок пока нет
- Inguinal Hernia by Dr. Reema - 2147Документ23 страницыInguinal Hernia by Dr. Reema - 2147Reema Haji AbdullahОценок пока нет
- 2019 Hernia Kuliah FKДокумент50 страниц2019 Hernia Kuliah FKKhairani NurhamidahОценок пока нет
- Hernia & PR: DR - Abdulwahid M Salih M.D. SurgeryДокумент38 страницHernia & PR: DR - Abdulwahid M Salih M.D. SurgeryumiumiОценок пока нет
- Inguinal Hernia EcaaДокумент36 страницInguinal Hernia EcaaElsha ZaskiaОценок пока нет
- DR - Niyan HerniaДокумент7 страницDR - Niyan HerniaDarawan MirzaОценок пока нет
- Hernia: Under Supervision DR Arzak SaberДокумент32 страницыHernia: Under Supervision DR Arzak Sabermathio medhatОценок пока нет
- HerniaДокумент47 страницHerniamalathiОценок пока нет
- Hernia: DR Teamir Negussie Assistant Professor Dept of SurgeryДокумент47 страницHernia: DR Teamir Negussie Assistant Professor Dept of SurgeryteamirОценок пока нет
- Hernia: Done by D1 GroupДокумент47 страницHernia: Done by D1 Groupanindyadputri100% (1)
- Hernia-Hx & PExДокумент5 страницHernia-Hx & PExShirline MillingtonОценок пока нет
- HerniaДокумент46 страницHerniaZubairkhan SuraniОценок пока нет
- Hernia 5mayДокумент28 страницHernia 5mayYeoh Shu TingОценок пока нет
- Testicular SwellingДокумент66 страницTesticular SwellingbrnardОценок пока нет
- Examination of The Abdomen: DR Elias M. (MD)Документ73 страницыExamination of The Abdomen: DR Elias M. (MD)ObsaОценок пока нет
- Submitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHДокумент26 страницSubmitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHKim BalacangОценок пока нет
- Anatomy of The Inguinal RegionДокумент24 страницыAnatomy of The Inguinal RegionAhmed ShehadaОценок пока нет
- HerniaДокумент67 страницHerniaياسر نعيم الربيعي100% (1)
- Key PointsДокумент34 страницыKey PointsSe YunОценок пока нет
- 1 Inguinal Hernia EditedДокумент34 страницы1 Inguinal Hernia EditedNadhirah ZulkifliОценок пока нет
- Inguinal HerniaДокумент6 страницInguinal HerniaignatiuserikОценок пока нет
- Part 2.herniaДокумент38 страницPart 2.herniaapi-19641337Оценок пока нет
- Acute AbdomenДокумент13 страницAcute AbdomenS SultanОценок пока нет
- HerniaДокумент62 страницыHerniaBen IntosiusОценок пока нет
- GI Exam (RCT)Документ6 страницGI Exam (RCT)kenners100% (11)
- Hernia: DR - Surender Singh DhankharДокумент36 страницHernia: DR - Surender Singh DhankharBharat BhushanОценок пока нет
- Hernia in ChildrenДокумент5 страницHernia in Childrensusheewa100% (1)
- Temporomandibular JointДокумент32 страницыTemporomandibular JointkikiОценок пока нет
- Short Case and Long Case by Dr. MurtozaДокумент79 страницShort Case and Long Case by Dr. Murtoza202Manjida Rahman OniОценок пока нет
- Hernia FinalДокумент21 страницаHernia FinalYeoh Shu TingОценок пока нет
- Abdominallecture 2015Документ103 страницыAbdominallecture 2015Abdelrahman MokhtarОценок пока нет
- CSS Hernia Inguinal RSAI Kel 8 EditДокумент33 страницыCSS Hernia Inguinal RSAI Kel 8 EditElsha ZaskiaОценок пока нет
- HERNIAДокумент39 страницHERNIAchebetnaomi945Оценок пока нет
- CSP Groin LumpДокумент39 страницCSP Groin LumpFebby ShabrinaОценок пока нет
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwДокумент51 страницаInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiОценок пока нет
- HerniasДокумент49 страницHerniasAliОценок пока нет
- Integrated Lectures, Year III Medical Students, Gulu University Medical SchoolДокумент15 страницIntegrated Lectures, Year III Medical Students, Gulu University Medical SchoolxilcomОценок пока нет
- Hernia1 InguinalДокумент7 страницHernia1 InguinalmunafalmahdiОценок пока нет
- Inguinal Hernia: Peritoneum, Resulting in A BulgeДокумент5 страницInguinal Hernia: Peritoneum, Resulting in A BulgeJunathan L. Delgado100% (1)
- 4-Systematic Surgery Abdominal HerniaДокумент44 страницы4-Systematic Surgery Abdominal HerniaabdisamedОценок пока нет
- Groin HerniaДокумент12 страницGroin HerniaAhmed Abdel-naserОценок пока нет
- HerniaДокумент26 страницHerniaSudhanshu ShekharОценок пока нет
- Assessment of MS SystemДокумент68 страницAssessment of MS Systemdileepkumar.duhs4817Оценок пока нет
- A.muskulo Skeletal Trauma Seminar UB (23okt2016)Документ67 страницA.muskulo Skeletal Trauma Seminar UB (23okt2016)Wahyuningsih HusainОценок пока нет
- Hemorrhoids: Ginesha Hafidzy GarishahДокумент35 страницHemorrhoids: Ginesha Hafidzy GarishahrizqinadiaОценок пока нет
- Acute Abdomen - DR Raya Batubara, SP.BДокумент39 страницAcute Abdomen - DR Raya Batubara, SP.BGJMasterОценок пока нет
- Hernia Scrotalis FIxДокумент56 страницHernia Scrotalis FIxivaniОценок пока нет
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (1)
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Meckel Diverticulum, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandMeckel Diverticulum, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesОт EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesРейтинг: 1 из 5 звезд1/5 (1)
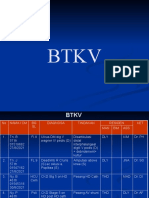
- Weekly BTKV 2 Sept 2021-1Документ14 страницWeekly BTKV 2 Sept 2021-1lsintaningtyasОценок пока нет
- Adjuvant Radiation Therapy in Breast Cancer .4Документ10 страницAdjuvant Radiation Therapy in Breast Cancer .4lsintaningtyasОценок пока нет
- Pi Is 2058534919300071Документ7 страницPi Is 2058534919300071lsintaningtyasОценок пока нет
- Deep Sternal Wound Infections: Evidence For Prevention, Treatment, and Reconstructive SurgeryДокумент12 страницDeep Sternal Wound Infections: Evidence For Prevention, Treatment, and Reconstructive Surgerylsintaningtyas100% (1)
- NewWeekly BTKV 26 Agustus 2021Документ9 страницNewWeekly BTKV 26 Agustus 2021lsintaningtyasОценок пока нет
- NewWeekly BTKV 26 Agustus 2021Документ9 страницNewWeekly BTKV 26 Agustus 2021lsintaningtyasОценок пока нет
- Carcinoma MammaenewДокумент48 страницCarcinoma MammaenewlsintaningtyasОценок пока нет
- 39 6 955Документ8 страниц39 6 955lsintaningtyasОценок пока нет
- AsianJNeurosurg13193-3029062 082450Документ3 страницыAsianJNeurosurg13193-3029062 082450lsintaningtyasОценок пока нет
- 21 Nov 2017Документ2 страницы21 Nov 2017lsintaningtyasОценок пока нет
- AsianJNeurosurg13193-3029062 082450Документ3 страницыAsianJNeurosurg13193-3029062 082450lsintaningtyasОценок пока нет
- New Text DocumentДокумент1 страницаNew Text DocumentlsintaningtyasОценок пока нет
- 6319 12310 2 PBДокумент8 страниц6319 12310 2 PBlsintaningtyasОценок пока нет
- Examination of Hernia: DR Min Oo SurgeryДокумент39 страницExamination of Hernia: DR Min Oo SurgerylsintaningtyasОценок пока нет
- HormoneДокумент68 страницHormonelsintaningtyasОценок пока нет
- Nuclear Receptors 2006Документ31 страницаNuclear Receptors 2006lsintaningtyasОценок пока нет
- Dsa 697Документ57 страницDsa 697lsintaningtyasОценок пока нет
- Hormone Action VIA Nuclear Receptors: Dr. Michal LahavДокумент31 страницаHormone Action VIA Nuclear Receptors: Dr. Michal LahavlsintaningtyasОценок пока нет
- Auricular Tissue Engineering Using Osteogenic.14Документ9 страницAuricular Tissue Engineering Using Osteogenic.14Maria Mercedes Rosales NuñezОценок пока нет
- Neo-Synephri Ne I Iot Ri Vi NДокумент38 страницNeo-Synephri Ne I Iot Ri Vi NMarlo Dañez NorbeОценок пока нет
- Focusing On Children Mental HealthДокумент2 страницыFocusing On Children Mental HealthDzatil HusniОценок пока нет
- Swollen Ankles and FeetДокумент36 страницSwollen Ankles and FeetMagikeyОценок пока нет
- Plagiarism Scan Report: Plagiarised Unique Words CharactersДокумент1 страницаPlagiarism Scan Report: Plagiarised Unique Words CharactersEunice TrinidadОценок пока нет
- Removing Contaminated Gown and Gloves ChecklistДокумент3 страницыRemoving Contaminated Gown and Gloves ChecklistFar Ri NaОценок пока нет
- Oral Mucosal Ulceration - A Clinician's Guide To Diagnosis and TreatmentДокумент9 страницOral Mucosal Ulceration - A Clinician's Guide To Diagnosis and TreatmentAnonymous pvuOXZОценок пока нет
- 2015 Peperiksaan Percubaan Bahasa Inggeris SPM Pulau Pinang Kertas 2Документ18 страниц2015 Peperiksaan Percubaan Bahasa Inggeris SPM Pulau Pinang Kertas 2Pete Wang83% (6)
- Geriatric ...... Dental CareДокумент39 страницGeriatric ...... Dental CareDelvine AderoОценок пока нет
- Incentive SpirometryДокумент5 страницIncentive Spirometryrachelmores12Оценок пока нет
- Ijdn - 2Документ14 страницIjdn - 2Dr Lalit Chandravanshi (SUSAH Associate Professor)Оценок пока нет
- Review: Detection & Diagnosis of Plant Leaf Disease Using Integrated Image Processing ApproachДокумент17 страницReview: Detection & Diagnosis of Plant Leaf Disease Using Integrated Image Processing ApproachdanangkitaОценок пока нет
- Butyl CellosolveДокумент1 страницаButyl CellosolvebiosaludquimicaОценок пока нет
- AHA18HyperPocketGuidePRINT3FINAL APPROVED PDFДокумент2 страницыAHA18HyperPocketGuidePRINT3FINAL APPROVED PDFAmanda JulianaОценок пока нет
- Research On DOH Approved Herbal MedicinesДокумент31 страницаResearch On DOH Approved Herbal Medicinesfilithesis79% (14)
- 2nd PU Practical Viva QuestionsДокумент10 страниц2nd PU Practical Viva QuestionsSadhvi CОценок пока нет
- Unicef in IndiaДокумент22 страницыUnicef in IndiaNamita Kothari100% (1)
- Covid-19: Asian Xenophobia and RacismДокумент12 страницCovid-19: Asian Xenophobia and RacismNayab Binte Fiaz100% (1)
- Phenacetin MsdsДокумент6 страницPhenacetin MsdstylerОценок пока нет
- Motion Is LotionДокумент2 страницыMotion Is LotionQing JyulyanОценок пока нет
- Early Considerations of Mental IllnessДокумент14 страницEarly Considerations of Mental Illnesszuh blackОценок пока нет
- Healthy Foods and The Body Parts They ResembleДокумент4 страницыHealthy Foods and The Body Parts They ResembleRobert AndujarОценок пока нет
- Project Proposal DsaДокумент2 страницыProject Proposal DsaChristine Joy Pellos MacabeoОценок пока нет
- ExodontiaДокумент32 страницыExodontiaahmed amerОценок пока нет
- 01a Calgary Cambridge Framework - BasicДокумент3 страницы01a Calgary Cambridge Framework - BasicJohn Sebastian Bittner SolisОценок пока нет
- 11 Nursing Care Pacemaker Emil 2019Документ5 страниц11 Nursing Care Pacemaker Emil 2019ameliajamirusОценок пока нет
- History of MicrobiologyДокумент23 страницыHistory of MicrobiologyISRAELОценок пока нет
- HPV Vaccination: It'S Us Against The Human PapillomavirusДокумент30 страницHPV Vaccination: It'S Us Against The Human Papillomavirussalam majzoubОценок пока нет
- Test 1 Part 1 TapecsriptДокумент19 страницTest 1 Part 1 TapecsriptMerryОценок пока нет
- Chemistry Assignment: Properties of NicotineДокумент10 страницChemistry Assignment: Properties of Nicotineharshitha jagathieshОценок пока нет