Вам также может понравиться
- The Dental Curing Light: Richard B. PriceДокумент20 страницThe Dental Curing Light: Richard B. PricepoojaОценок пока нет
- Light Curing in Orthodontics Should We Be Concerned?: Neil MccuskerДокумент6 страницLight Curing in Orthodontics Should We Be Concerned?: Neil MccuskerRohan BhagatОценок пока нет
- Radiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental AcademyДокумент85 страницRadiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- EXPERIMENT 1: Laser Safety D: Never Allow A Laser Beam To Enter The Eye!Документ14 страницEXPERIMENT 1: Laser Safety D: Never Allow A Laser Beam To Enter The Eye!Ali AmjadОценок пока нет
- Dental Light Curing— Assessing The Blue LighДокумент14 страницDental Light Curing— Assessing The Blue LighCh BilalОценок пока нет
- Lasers in Conservative Dentistry: An Overview: Abst TДокумент4 страницыLasers in Conservative Dentistry: An Overview: Abst TCharu Kapur ChhabraОценок пока нет
- Draft BIR Shielding Book June99tДокумент85 страницDraft BIR Shielding Book June99tpontypool111Оценок пока нет
- Applications of Radiant Energy Eye ProtectionДокумент1 страницаApplications of Radiant Energy Eye ProtectionreacharunkОценок пока нет
- Laser Radiation HazardsДокумент16 страницLaser Radiation HazardsLarryKnappОценок пока нет
- Initial Fracture Resistance and Curing Temperature Rise of Ten Contemporary Resin-Based Composites With Increasing Radiant ExposureДокумент9 страницInitial Fracture Resistance and Curing Temperature Rise of Ten Contemporary Resin-Based Composites With Increasing Radiant ExposureheycoolalexОценок пока нет
- Short All 2013Документ9 страницShort All 2013JumanjiОценок пока нет
- OSRAM Infrared IR Vision Eye SafetyДокумент9 страницOSRAM Infrared IR Vision Eye SafetyJossueОценок пока нет
- International Journal of Computational Engineering Research (IJCER)Документ7 страницInternational Journal of Computational Engineering Research (IJCER)International Journal of computational Engineering research (IJCER)Оценок пока нет
- 120kv 350masДокумент85 страниц120kv 350masKilat Permana Komenk100% (1)
- Eye Safety of IREDsДокумент17 страницEye Safety of IREDsЕвгений МихайловОценок пока нет
- Application Note Eye Safety of IREDs Used in Lamp ApplicationsДокумент9 страницApplication Note Eye Safety of IREDs Used in Lamp ApplicationsMariz MallonОценок пока нет
- Radiation ProtectionДокумент20 страницRadiation Protectionaiimsjdh acadОценок пока нет
- Dental Xray FactsДокумент13 страницDental Xray FactsEndah RahayuОценок пока нет
- FTA ReportДокумент20 страницFTA Reportzen AlkaffОценок пока нет
- Evaluating Blue-Light HazardДокумент11 страницEvaluating Blue-Light HazardSilvioGlasgow100% (1)
- The Light-Curing Unit: An Essential Piece of Dental EquipmentДокумент11 страницThe Light-Curing Unit: An Essential Piece of Dental EquipmentViC JasonОценок пока нет
- 2 Kenji Shimokawa 2018 Effect of Light Curing Units On The Polymerization of Bulk Fill Resin-Based Composites.Документ11 страниц2 Kenji Shimokawa 2018 Effect of Light Curing Units On The Polymerization of Bulk Fill Resin-Based Composites.Alejandra Herrera BarreraОценок пока нет
- UVC LEDs For DisinfectionДокумент12 страницUVC LEDs For Disinfectionfudfudfud100% (1)
- equiДокумент7 страницequisanyengereОценок пока нет
- Introduction To Laser Safety - Unit 01Документ90 страницIntroduction To Laser Safety - Unit 01TEBATSOОценок пока нет
- Contemporary Issues in Light Curing: Literature ReviewДокумент11 страницContemporary Issues in Light Curing: Literature ReviewpoojaОценок пока нет
- Dental Light CuringДокумент14 страницDental Light Curingrohan badgujarОценок пока нет
- Guidance Radiation Risk Assessment For Work With X-Rays 24-06-2021Документ31 страницаGuidance Radiation Risk Assessment For Work With X-Rays 24-06-2021Rafa PopocaОценок пока нет
- Science Written Works q2Документ3 страницыScience Written Works q2Erich Benedict ClerigoОценок пока нет
- Non-Ionizing Radiation GuideДокумент10 страницNon-Ionizing Radiation GuidemohamedОценок пока нет
- ACFrOgD K2syqYdzGmMfJF - lPyYf1oVfDjphAwuk7P0lWGdwFXbdZIXMsQ7 HfsuH81sXgPMFWyGUV41UU0auphmaWXZtBQ1hobRRQO0LE Zzowz3DZwbwR1KIXH GEДокумент26 страницACFrOgD K2syqYdzGmMfJF - lPyYf1oVfDjphAwuk7P0lWGdwFXbdZIXMsQ7 HfsuH81sXgPMFWyGUV41UU0auphmaWXZtBQ1hobRRQO0LE Zzowz3DZwbwR1KIXH GEPriscilla Bandeira FrotaОценок пока нет
- Radiation Safety Distance-NDE SMEДокумент37 страницRadiation Safety Distance-NDE SME庄查理Оценок пока нет
- Sunscreen Guide Explains Key ConceptsДокумент121 страницаSunscreen Guide Explains Key ConceptsRizweta DestinОценок пока нет
- RADTECH - Glossary of TermsДокумент6 страницRADTECH - Glossary of TermsjlbbcoelhoОценок пока нет
- Proteksi Radiasi Dari RadiografiДокумент34 страницыProteksi Radiasi Dari RadiografiBachtiar Muhammad ArifОценок пока нет
- Laser Safety Document OverviewДокумент80 страницLaser Safety Document OverviewriomjОценок пока нет
- Technical Climaguard Us Technical-Reference-Guide 0619Документ20 страницTechnical Climaguard Us Technical-Reference-Guide 0619karim FathallahОценок пока нет
- 6840 27220 1 PBДокумент3 страницы6840 27220 1 PBPercy Andree Bayona GuillermoОценок пока нет
- An Introduction To FluorescenceДокумент36 страницAn Introduction To FluorescenceFrank LaporteОценок пока нет
- 2011 Glare J.SolarEnergyEngr Vol133Документ9 страниц2011 Glare J.SolarEnergyEngr Vol133hafizh abiyyuОценок пока нет
- Protecting Your Laser DiodeДокумент30 страницProtecting Your Laser DiodebseptrianiОценок пока нет
- Safe Use of RadiationsДокумент18 страницSafe Use of RadiationsMohsin AliОценок пока нет
- Dental Radiation Safety GuideДокумент43 страницыDental Radiation Safety GuideFaye Nervanna Alecha AlferezОценок пока нет
- Hazards of Operating Machine Sources of X-Rays: Environmental Health & SafetyДокумент3 страницыHazards of Operating Machine Sources of X-Rays: Environmental Health & SafetyjojokawayОценок пока нет
- Dxa ShieldingДокумент21 страницаDxa ShieldingGeorgiana KokonaОценок пока нет
- Radiometric vs Photometric MeasurementsДокумент9 страницRadiometric vs Photometric Measurementsoscar_sm77Оценок пока нет
- TNT 01-1 PDFДокумент4 страницыTNT 01-1 PDFJose J. NuñezОценок пока нет
- Examen Ambrosio 2 InglesДокумент12 страницExamen Ambrosio 2 InglesLadhy Guadalupe Feliciano FuentesОценок пока нет
- Physics Researchhh )Документ3 страницыPhysics Researchhh )Jairus MalloОценок пока нет
- Unit1pptnotes 210823071031Документ65 страницUnit1pptnotes 210823071031SAMPATH AОценок пока нет
- Stability of The Light Output, Oral Cavity Tip Accessibility in Posterior Region and Emission Spectrum of Light-Curing UnitsДокумент10 страницStability of The Light Output, Oral Cavity Tip Accessibility in Posterior Region and Emission Spectrum of Light-Curing UnitspoojaОценок пока нет
- Cell Phone and Tower Radiation HazardsДокумент50 страницCell Phone and Tower Radiation HazardsVarun GuptaОценок пока нет
- Laser Module 2Документ24 страницыLaser Module 2Luis Enrique B GОценок пока нет
- 255 Basic Principles of Laser TechnologyДокумент9 страниц255 Basic Principles of Laser TechnologyMatch BoxОценок пока нет
- CBM355 Medical Imaging Systems 2-MarksДокумент23 страницыCBM355 Medical Imaging Systems 2-Markssanthosh sekar100% (2)
- Radiation ShieldingДокумент28 страницRadiation ShieldingJayath BogahawatteОценок пока нет
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)От EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)Оценок пока нет
- Impacted Incisors GuidelinesДокумент13 страницImpacted Incisors GuidelinesSadaf AhmedОценок пока нет
- Step-By-Step For CEREC: Preparation CAD/CAM Process Try-InДокумент2 страницыStep-By-Step For CEREC: Preparation CAD/CAM Process Try-InMichael XuОценок пока нет
- Dental Practitioner: Proposal For Dental Indemnity PolicyДокумент9 страницDental Practitioner: Proposal For Dental Indemnity PolicyMichael XuОценок пока нет
- Impacted Incisors GuidelinesДокумент13 страницImpacted Incisors GuidelinesSadaf AhmedОценок пока нет
- Beck CD A Journal Pinhole Article October 20181Документ5 страницBeck CD A Journal Pinhole Article October 20181Michael XuОценок пока нет
- PB201705-105 Membership Benefits Handbook 2017-18Документ48 страницPB201705-105 Membership Benefits Handbook 2017-18Michael XuОценок пока нет
- Beck CD A Journal Pinhole Article October 20181Документ5 страницBeck CD A Journal Pinhole Article October 20181Michael XuОценок пока нет
- 17 1195 Consumer Epic WhiteningДокумент2 страницы17 1195 Consumer Epic WhiteningMichael XuОценок пока нет
- 179-Article Text-302-1-10-20171121 PDFДокумент5 страниц179-Article Text-302-1-10-20171121 PDFMichael XuОценок пока нет
- Seminar Evaluation Form - Minimax ImplantДокумент1 страницаSeminar Evaluation Form - Minimax ImplantMichael XuОценок пока нет
- Supernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportДокумент4 страницыSupernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportMichael XuОценок пока нет
- 2016 Waterlase PEDOДокумент2 страницы2016 Waterlase PEDOMichael XuОценок пока нет
- Adhesive Restorations, Centric Relation and The Dahl PrincipleДокумент15 страницAdhesive Restorations, Centric Relation and The Dahl PrincipleJorge RojasОценок пока нет
- IPS E-Max Clinical Guide PDFДокумент44 страницыIPS E-Max Clinical Guide PDFKarolis KОценок пока нет
- 17 1195 Consumer Epic PainTherapyДокумент2 страницы17 1195 Consumer Epic PainTherapyMichael XuОценок пока нет
- QZAДокумент52 страницыQZAMichael XuОценок пока нет
- A Polycromatic Composite Layering Approach For Solving A Complex Class IV Direct Venner Diastema Combination Part 1Документ6 страницA Polycromatic Composite Layering Approach For Solving A Complex Class IV Direct Venner Diastema Combination Part 1Michael XuОценок пока нет
- Digital Dentistry Sydney 2020Документ13 страницDigital Dentistry Sydney 2020Michael XuОценок пока нет
- A Deprogrammer For Occlusal Analysis and Simplified Accurate Case MountingДокумент7 страницA Deprogrammer For Occlusal Analysis and Simplified Accurate Case MountingMichael XuОценок пока нет
- Dental Ceramics For Restoration and Metal VeneeringДокумент23 страницыDental Ceramics For Restoration and Metal VeneeringMichael XuОценок пока нет
- 10 Reasons Why: Orthodontics Isn't As Hard As You ThinkДокумент14 страниц10 Reasons Why: Orthodontics Isn't As Hard As You ThinkMichael XuОценок пока нет
- Impacted Incisors GuidelinesДокумент13 страницImpacted Incisors GuidelinesSadaf AhmedОценок пока нет
- Fluoride Varnish Instructions From NT Healthy SmilesДокумент17 страницFluoride Varnish Instructions From NT Healthy SmilesMichael XuОценок пока нет
- The 3 Procedures Dentists Must KnowДокумент10 страницThe 3 Procedures Dentists Must KnowMichael XuОценок пока нет
- Clinical Performance of Cervical Restorations With Desensitizing Agents - 18-Month Clinical TrialДокумент7 страницClinical Performance of Cervical Restorations With Desensitizing Agents - 18-Month Clinical TrialMichael XuОценок пока нет
- Local Anesthesia and Med Compromised Pts Jcda 2000Документ13 страницLocal Anesthesia and Med Compromised Pts Jcda 2000Michael XuОценок пока нет
- Good Occlusal Practice in Advanced Restorative DentistryДокумент10 страницGood Occlusal Practice in Advanced Restorative DentistryMichael XuОценок пока нет
- 1 s2.0 S0011853211000346 Main PDFДокумент6 страниц1 s2.0 S0011853211000346 Main PDFMichael XuОценок пока нет
- CBCT Scanners For The General Dental OfficeДокумент15 страницCBCT Scanners For The General Dental OfficeMichael Xu100% (1)
- Thesis TopicДокумент3 страницыThesis TopicLens NewОценок пока нет
- Catalogo de SuperCapacitores PDFДокумент2 страницыCatalogo de SuperCapacitores PDFgvidal_7777Оценок пока нет
- Renewable Train and Railway Station: Kaustubh Dilip Patil, Uday R. Patil, Firoj U. PathanДокумент5 страницRenewable Train and Railway Station: Kaustubh Dilip Patil, Uday R. Patil, Firoj U. PathanFirozPathanОценок пока нет
- Pgstat100n DownloadДокумент7 страницPgstat100n DownloadAgus JatmikoОценок пока нет
- Power Quality Problems and New SolutionsДокумент9 страницPower Quality Problems and New SolutionsSing-Yew LAMОценок пока нет
- Design of A Photovoltaic System With Ultracapacitor Energy Buffer Design of A Photovoltaic System With Ultracapacitor Energy BufferДокумент8 страницDesign of A Photovoltaic System With Ultracapacitor Energy Buffer Design of A Photovoltaic System With Ultracapacitor Energy BufferAbdoooОценок пока нет
- Energies: The Role of Supercapacitors in Regenerative Braking SystemsДокумент15 страницEnergies: The Role of Supercapacitors in Regenerative Braking SystemsHua Hidari YangОценок пока нет
- A Review Study On Energy Harvesting Systems For Vehicles: Umut Aksu, Recep HaliciogluДокумент9 страницA Review Study On Energy Harvesting Systems For Vehicles: Umut Aksu, Recep HalicioglusahayaОценок пока нет
- 000000000001008852Документ102 страницы000000000001008852komal_8859Оценок пока нет
- Optimisation of Fuel Cell and Supercapacitors in ElectricДокумент38 страницOptimisation of Fuel Cell and Supercapacitors in ElectricNithin JohnОценок пока нет
- Super CapacitorsДокумент23 страницыSuper CapacitorsKVVОценок пока нет
- Applied Surface Science: Chen Hao, Xiaokun Wang, Xingli Wu, Yaning Guo, Linli Zhu, Xiaohong WangДокумент3 страницыApplied Surface Science: Chen Hao, Xiaokun Wang, Xingli Wu, Yaning Guo, Linli Zhu, Xiaohong Wangreca adiyanti rahmanОценок пока нет
- EV (Advance) Objectives - 23385812 - 2023 - 09 - 27 - 20 - 13Документ9 страницEV (Advance) Objectives - 23385812 - 2023 - 09 - 27 - 20 - 13priyanshuraj2379Оценок пока нет
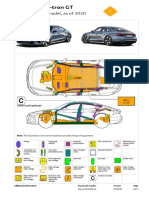
- Audi Rescue Data Sheets (E-Tron GT - Sportback - 2020 - 5d - Electric - EN)Документ4 страницыAudi Rescue Data Sheets (E-Tron GT - Sportback - 2020 - 5d - Electric - EN)caragan1970Оценок пока нет
- Development of Electric Vehicle Powertrain: Experimental Implementation and Performance AssessmentДокумент7 страницDevelopment of Electric Vehicle Powertrain: Experimental Implementation and Performance AssessmentBaldau Pratap Singh BundelaОценок пока нет
- Abstract Book - ICFME-2022Документ105 страницAbstract Book - ICFME-2022S R E E N I V A S AОценок пока нет
- Supercapacitor PHD ThesisДокумент8 страницSupercapacitor PHD Thesispuzinasymyf3100% (2)
- ORO551 Renewable Energy Sources QB 2Документ7 страницORO551 Renewable Energy Sources QB 2Nallappan Rajj AОценок пока нет
- Review On Conducting Polymers and Their ApplicationsДокумент15 страницReview On Conducting Polymers and Their ApplicationsS POORNIMAОценок пока нет
- Nanotechnology ApplicationsДокумент13 страницNanotechnology ApplicationsSuseel Jai KrishnanОценок пока нет
- Ev Battery TechnlogoiesДокумент91 страницаEv Battery TechnlogoiesAtheli Vijay ChandraОценок пока нет
- Design and Fabrication of Basic Electric F1 Racing CarДокумент9 страницDesign and Fabrication of Basic Electric F1 Racing CarPushpak N UmaleОценок пока нет
- Seminar Report PAPER BATTERY (2016-20)Документ24 страницыSeminar Report PAPER BATTERY (2016-20)Waquar Ahmad90% (20)
- Waste Management: Samane Maroufi, Mohannad Mayyas, Veena SahajwallaДокумент7 страницWaste Management: Samane Maroufi, Mohannad Mayyas, Veena SahajwallaCristina VladutaОценок пока нет
- Graphene Catalogue2019Документ72 страницыGraphene Catalogue2019Ana Clara SoaresОценок пока нет
- Energy Storage Devices in Electrified Railway Systems Liu LiДокумент19 страницEnergy Storage Devices in Electrified Railway Systems Liu LiDaniel ChamposkiОценок пока нет
- Supercapacitors Energy Storage SystemДокумент1 страницаSupercapacitors Energy Storage SystemNithya Susan VargheseОценок пока нет
- Teste 9º AnoДокумент5 страницTeste 9º Anomanuela.ines.vaz1068Оценок пока нет
- Multifunctional Composites For Future Energy Storage in Aerospace StructuresДокумент21 страницаMultifunctional Composites For Future Energy Storage in Aerospace StructureshijerОценок пока нет
- Future Storage PDFДокумент7 страницFuture Storage PDFTown Obio EteteОценок пока нет