Вам также может понравиться
- AntidotesДокумент36 страницAntidotesMohamed Haggag100% (1)
- Medication Administration PolicyДокумент188 страницMedication Administration Policyليراث ليОценок пока нет
- Intake and Output ChartДокумент2 страницыIntake and Output ChartViral Chann3LОценок пока нет
- Amrita Hospital VTE Form Assesses Patient RiskДокумент2 страницыAmrita Hospital VTE Form Assesses Patient RiskNatasha BhasinОценок пока нет
- Forms BДокумент14 страницForms BDaryl Joshua SaturnoОценок пока нет
- KARDEXДокумент4 страницыKARDEXDaniel GalitzineОценок пока нет
- 01 Nursing Note SampleДокумент1 страница01 Nursing Note Sampletesttest testОценок пока нет
- Vascularaccess 508 PDFДокумент4 страницыVascularaccess 508 PDFVina YuwandaОценок пока нет
- Intravenous CannulationДокумент9 страницIntravenous CannulationjeorjОценок пока нет
- Adult Assessment Tool 2014Документ8 страницAdult Assessment Tool 2014Charm PradoОценок пока нет
- TB QuestionnaireДокумент1 страницаTB QuestionnaireaplesgjskОценок пока нет
- Abbreviations ListДокумент6 страницAbbreviations ListolivedaisychainОценок пока нет
- C 13Документ11 страницC 13Jo100% (1)
- Advanced Airway Care: Intensive Care Unit PerspectiveДокумент42 страницыAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- IBE, Susanna Martha B. 2014-57561 Ward 1Документ4 страницыIBE, Susanna Martha B. 2014-57561 Ward 1WazzupОценок пока нет
- Patient Monitoring SheetДокумент8 страницPatient Monitoring SheetAndrea Sibayan SorianoОценок пока нет
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFДокумент90 страницIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataОценок пока нет
- Heparin Drip Calculation ReferenceДокумент1 страницаHeparin Drip Calculation ReferencePranabh KushwahaОценок пока нет
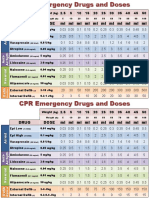
- CPR Emergency Drug DosesДокумент2 страницыCPR Emergency Drug DosesCote ParejaОценок пока нет
- Blood TransfusionДокумент18 страницBlood TransfusionJeeduu frostОценок пока нет
- Fundamentals of Nursing Lecture Notes PDF - CompressДокумент43 страницыFundamentals of Nursing Lecture Notes PDF - CompressFelyn DavideОценок пока нет
- Criticalcaredrugs 2 PDFДокумент2 страницыCriticalcaredrugs 2 PDFabdallahОценок пока нет
- Blood Transfusions - TGH Policies & ProceduresДокумент4 страницыBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoОценок пока нет
- Study Vital Signs ProtocolДокумент3 страницыStudy Vital Signs ProtocolHariprasathОценок пока нет
- Physical Assessment ChecklistДокумент1 страницаPhysical Assessment ChecklistDMRMОценок пока нет
- VTE Risk AssessmentДокумент2 страницыVTE Risk AssessmentpriyopanjiОценок пока нет
- Integrated ChecklistДокумент2 страницыIntegrated ChecklistKena BenОценок пока нет
- Blood Transfusion Single Use PathwayДокумент6 страницBlood Transfusion Single Use PathwayropusanОценок пока нет
- Blood Administration: NRS 108 Essec County CollegeДокумент22 страницыBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniОценок пока нет
- Changing Position of A Helpless PatientДокумент14 страницChanging Position of A Helpless PatientKartick DeyОценок пока нет
- Managing corticosteroids and their side effectsДокумент6 страницManaging corticosteroids and their side effectsKrista Madranca CastroОценок пока нет
- Medication Administration WorksheetДокумент6 страницMedication Administration WorksheetCheska CarrionОценок пока нет
- RECOVER Initiative CPR Reporting Sheet 2020. v3.2Документ2 страницыRECOVER Initiative CPR Reporting Sheet 2020. v3.2Mohana Preethi MОценок пока нет
- Pre-op Evaluation SummaryДокумент1 страницаPre-op Evaluation Summarysabbo morsОценок пока нет
- Drug CalculationsДокумент2 страницыDrug CalculationsBern NerquitОценок пока нет
- Post OpДокумент6 страницPost OpFrinkaWijayaОценок пока нет
- Drugs in Cardiac EnmergenciesДокумент94 страницыDrugs in Cardiac EnmergenciesVijayan VelayudhanОценок пока нет
- High Risk Consent For PCIДокумент1 страницаHigh Risk Consent For PCISree Sowjanya PatibandlaОценок пока нет
- PERIOPERATIVE NURSING PHASESДокумент11 страницPERIOPERATIVE NURSING PHASESDa BondadОценок пока нет
- Bioinstrumentation II: Lecture 4: ECG MachineДокумент30 страницBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaОценок пока нет
- Percentage BMI calculator helps determine patient weight statusДокумент36 страницPercentage BMI calculator helps determine patient weight statuskasonde.musonda8Оценок пока нет
- Maste Med SheetДокумент78 страницMaste Med SheetBarbie Wiggers100% (1)
- Cardiac Stent PriceДокумент4 страницыCardiac Stent PriceMahmudul Hasan TusharОценок пока нет
- Vital Signs Monitoring SheetДокумент4 страницыVital Signs Monitoring SheetDenvicОценок пока нет
- Nursing Dummy ChartДокумент4 страницыNursing Dummy Chartis_aradanasОценок пока нет
- Sepsis Recognition and TreatmentДокумент33 страницыSepsis Recognition and TreatmentNhat NguyenОценок пока нет
- 2 Fluid and Electrolyte AbnormalityДокумент16 страниц2 Fluid and Electrolyte AbnormalityGoez Aditya NugrahaОценок пока нет
- Nursing Assessment ToolДокумент6 страницNursing Assessment ToolRaniОценок пока нет
- Plymouth Hospitals Guide to Nasogastric and Gastrostomy FeedingДокумент45 страницPlymouth Hospitals Guide to Nasogastric and Gastrostomy FeedingbandarascbОценок пока нет
- Banana Leaf Dressing For Partial Thickness WoundsДокумент6 страницBanana Leaf Dressing For Partial Thickness Woundsapi-3801331100% (1)
- Care Plan TemplateДокумент12 страницCare Plan TemplateemipОценок пока нет
- Nutritional Management of Renal DiseasesДокумент3 страницыNutritional Management of Renal Diseasescbac1990Оценок пока нет
- Emergency Department Intubation ChecklisTДокумент2 страницыEmergency Department Intubation ChecklisTStacey Woods100% (1)
- Medication Adherence Questionnaire (MAQ) : ARMS ScaleДокумент4 страницыMedication Adherence Questionnaire (MAQ) : ARMS ScaleEnesaHodžićОценок пока нет
- Blood Transfusion GuideДокумент28 страницBlood Transfusion GuideChristina DienteОценок пока нет
- Blood Transfusion: Etiology of Blood CellДокумент4 страницыBlood Transfusion: Etiology of Blood Cellbunso padillaОценок пока нет
- Irene's Flow SheetДокумент1 страницаIrene's Flow SheetmrpatrickrnОценок пока нет
- Night BeforeДокумент3 страницыNight BeforeChris MoffettОценок пока нет
- Fall Risk Assessment FormДокумент3 страницыFall Risk Assessment FormMichael Silva100% (1)
- Therapeutic Guidelines in Systemic Fungal Infection 3edДокумент127 страницTherapeutic Guidelines in Systemic Fungal Infection 3eddohuutri66Оценок пока нет
- AsqeДокумент11 страницAsqebrigde_xОценок пока нет
- Managing Diphtheria Cases and OutbreaksДокумент11 страницManaging Diphtheria Cases and Outbreaksbrigde_xОценок пока нет
- Adult and Adolescent GLДокумент287 страницAdult and Adolescent GLbrigde_xОценок пока нет
- The Changing Role of Beta-Blocker Therapy in Patients With CirrhosisДокумент4 страницыThe Changing Role of Beta-Blocker Therapy in Patients With Cirrhosisbrigde_xОценок пока нет
- Trombocitopenia PDFДокумент11 страницTrombocitopenia PDFbrigde_xОценок пока нет
- Xodo Document - Periprocedural - Anticoagulation - GuidelineДокумент16 страницXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xОценок пока нет
- 2011 Anticoagulant Pocket GuideДокумент4 страницы2011 Anticoagulant Pocket GuideDragoljubJesenicОценок пока нет
- Konjungtivitis Gonore Pada BayiДокумент16 страницKonjungtivitis Gonore Pada Bayibrigde_xОценок пока нет
- Anti Platelet PreopДокумент6 страницAnti Platelet Preopbrigde_xОценок пока нет
- Dengue EncephalopathyДокумент2 страницыDengue EncephalopathyIndra IhsanОценок пока нет
- Phlebotomy ProceduresДокумент67 страницPhlebotomy Proceduresadadan100% (1)
- Abses HatiДокумент6 страницAbses HatiGilang Haliza100% (1)
- 2011 ITP Pocket GuideДокумент8 страниц2011 ITP Pocket GuidevtОценок пока нет
- AIH2010Документ31 страницаAIH2010Irina GîrleanuОценок пока нет
- Manual NephrologyДокумент25 страницManual Nephrologybrigde_xОценок пока нет
- 16 ICUInsulinOrdersДокумент2 страницы16 ICUInsulinOrdersJahangir AlamОценок пока нет
- HistoryandPhysicalExamДокумент105 страницHistoryandPhysicalExamsilentscream0618Оценок пока нет
- Hyperglycemic Crises in DiabetesДокумент9 страницHyperglycemic Crises in DiabetesAhmad Barrun NidhomОценок пока нет
- The DASH Eating Plan: Lower Blood Pressure with DietДокумент24 страницыThe DASH Eating Plan: Lower Blood Pressure with DietLeslie Luján100% (1)
- 4 Possible Hemodynamic Profiles of HF: Congestion at RestДокумент6 страниц4 Possible Hemodynamic Profiles of HF: Congestion at Restbrigde_xОценок пока нет
- A LF EnhancedДокумент88 страницA LF Enhancedshadow1704Оценок пока нет
- KDIGO AKI Guideline DownloadДокумент141 страницаKDIGO AKI Guideline DownloadSandi AuliaОценок пока нет
- Basic Concepts of Fluid and Electrolyte TherapyДокумент136 страницBasic Concepts of Fluid and Electrolyte Therapynoorgianilestari100% (2)
- Abses HatiДокумент6 страницAbses HatiGilang Haliza100% (1)
- BMJ IrcДокумент6 страницBMJ IrcPaz RuizОценок пока нет
- American Journal of Kidney DiseasesДокумент93 страницыAmerican Journal of Kidney DiseasesBiw OnthebeachОценок пока нет
- 003 Clinical Appraisal-1Документ3 страницы003 Clinical Appraisal-1Erryl Justine AdvinculaОценок пока нет
- Depression Treatments in Dementia PatientsДокумент12 страницDepression Treatments in Dementia PatientsRiie Napabii DuatigasembilandelapanОценок пока нет
- B 2d Task AnalysisДокумент2 страницыB 2d Task Analysisapi-513861322Оценок пока нет
- Physical Examination by DRДокумент25 страницPhysical Examination by DRapi-3739910100% (2)
- The Adult Chain of Survival Module1Документ1 страницаThe Adult Chain of Survival Module1Mariam E.Оценок пока нет
- Gi 3Документ25 страницGi 3api-26938624Оценок пока нет
- Hydro Treatments TariffsДокумент2 страницыHydro Treatments TariffsLouvern MoodleyОценок пока нет
- Apixaban in Patients With Atrial FibrillationДокумент12 страницApixaban in Patients With Atrial FibrillationthedancingseaОценок пока нет
- Anesthesiology 1Документ59 страницAnesthesiology 1dagmawi girmaОценок пока нет
- LMTДокумент6 страницLMTMostafa AdamОценок пока нет
- Indapamide: M. Chajjman, R.C. Heel, R.N. Brogden, T.M. SpeightДокумент47 страницIndapamide: M. Chajjman, R.C. Heel, R.N. Brogden, T.M. SpeightFitria SalsabilaОценок пока нет
- Protonix (Pantoprazole)Документ1 страницаProtonix (Pantoprazole)EОценок пока нет
- V. AzapironesДокумент2 страницыV. AzapironesChristine Pialan SalimbagatОценок пока нет
- Medical History Taking Study GuideДокумент6 страницMedical History Taking Study GuideSarra Mood ImanОценок пока нет
- Progessence Phyto Plus: Essential Oil BlendДокумент2 страницыProgessence Phyto Plus: Essential Oil BlendJesh GranadoОценок пока нет
- ASAM Application Guidance 8 2019Документ22 страницыASAM Application Guidance 8 2019Victor Daniel Rivera Carrion100% (1)
- Peptic UlcerДокумент7 страницPeptic UlcerMonica Lauretta Sembiring0% (1)
- Covid 19 Fiqh Q & A Revised Edition Datuk DR Zulkifli Mohamad Al PDFДокумент201 страницаCovid 19 Fiqh Q & A Revised Edition Datuk DR Zulkifli Mohamad Al PDFhedar02Оценок пока нет
- Anemia: Causes, Symptoms and TreatmentДокумент2 страницыAnemia: Causes, Symptoms and TreatmentLazeh MeОценок пока нет
- DSPS - ScaleДокумент3 страницыDSPS - Scalekashyapi thakuriaОценок пока нет
- Onychomycosis Caused by Rare Fungus Phialophora jeanselmeiДокумент9 страницOnychomycosis Caused by Rare Fungus Phialophora jeanselmeiPande Agung MahariskiОценок пока нет
- Chronic Pain SyndromeДокумент1 страницаChronic Pain SyndromeAdvance Pain CareОценок пока нет
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Документ39 страницWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaОценок пока нет
- E. Legal Aspects of PharmacologyДокумент29 страницE. Legal Aspects of PharmacologyTricia Mae BayubayОценок пока нет
- Organization Chart and Services of Acworth Municipal HospitalДокумент6 страницOrganization Chart and Services of Acworth Municipal Hospitaltops123Оценок пока нет
- Othello SyndomeДокумент14 страницOthello SyndomeMuhammad IlhaamОценок пока нет
- Diabetic Coma in Type 2 DiabetesДокумент4 страницыDiabetic Coma in Type 2 DiabetesGilda Ditya AsmaraОценок пока нет
- Hem OccultДокумент2 страницыHem OccultfidofidzОценок пока нет
- The Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaeДокумент11 страницThe Efficacy of Acupuncture in The Treatment of Bell's Palsy Sequelaeseptiani hasibuanОценок пока нет
- Type 1 Diabetes OutlineДокумент2 страницыType 1 Diabetes OutlineDominique PorterОценок пока нет