Вам также может понравиться
- 1 Introduction To SpiritualityДокумент61 страница1 Introduction To Spiritualityharoon_kaziОценок пока нет
- Spirituality The Neglected Dimension of Holistic Mental Health Care 2012 PROQUESTДокумент6 страницSpirituality The Neglected Dimension of Holistic Mental Health Care 2012 PROQUESTDiego BolívarОценок пока нет
- Healing, Spirituality and Integrative Medicine: David M. Steinhorn, Jana Din, Angela JohnsonДокумент11 страницHealing, Spirituality and Integrative Medicine: David M. Steinhorn, Jana Din, Angela JohnsonTibor GalacziОценок пока нет
- Influence of Religious Beliefs On Healthcare PracticeДокумент12 страницInfluence of Religious Beliefs On Healthcare PracticeTemesgen EndalewОценок пока нет
- Professional Chaplaincy Its Role and Importance inДокумент17 страницProfessional Chaplaincy Its Role and Importance ineric_busse_1Оценок пока нет
- HHS Public Access: Incorporating Spirituality in Primary CareДокумент14 страницHHS Public Access: Incorporating Spirituality in Primary CareTibor GalacziОценок пока нет
- J Holist Nurs 2012 Barss 24 34Документ12 страницJ Holist Nurs 2012 Barss 24 34KholikОценок пока нет
- Therapy, Ideology, and Social Change: Mental Healing in Urban GhanaОт EverandTherapy, Ideology, and Social Change: Mental Healing in Urban GhanaОценок пока нет
- 1 s2.0 S0885392417302920 MainДокумент13 страниц1 s2.0 S0885392417302920 MainXavi Alsina CaulasОценок пока нет
- Chaplaincy Role Importance Health Care Sec1 WhitepaperДокумент4 страницыChaplaincy Role Importance Health Care Sec1 Whitepaperapi-292896527Оценок пока нет
- Thorensen, Spirituality - Health, AnnBehMed, 2002Документ11 страницThorensen, Spirituality - Health, AnnBehMed, 2002Roberto SollaОценок пока нет
- 1 Introduction To Spirituality PDFДокумент61 страница1 Introduction To Spirituality PDFSwami Gurunand50% (2)
- Private Prayer As A Suitable Intervention For Hospitalised Patients: A Critical Review of The LiteratureДокумент16 страницPrivate Prayer As A Suitable Intervention For Hospitalised Patients: A Critical Review of The LiteratureMircea PocolОценок пока нет
- Print APT 2002 Culliford 249 58Документ14 страницPrint APT 2002 Culliford 249 58elvineОценок пока нет
- Spiritual Care: Moving From Liminal Space' To Recognition: Coralie KingstonДокумент7 страницSpiritual Care: Moving From Liminal Space' To Recognition: Coralie KingstonNayr AirotcivОценок пока нет
- Final Research Paper Draft - AllenДокумент18 страницFinal Research Paper Draft - Allenapi-583318017Оценок пока нет
- Folk Wisdom and Traditional Healing Practices: Some Lessons For Modern PsychotherapiesДокумент20 страницFolk Wisdom and Traditional Healing Practices: Some Lessons For Modern PsychotherapiesPappoo KothariОценок пока нет
- Mark & Lyons, 2010Документ9 страницMark & Lyons, 2010Isaac James BisharaОценок пока нет
- Spiritual Care and The Role of Advanced Practice Nurses: Ahtisham YounasДокумент7 страницSpiritual Care and The Role of Advanced Practice Nurses: Ahtisham YounasGaela Leniel NocidalОценок пока нет
- Combining Stories: Reading Tibetan Medicine As A Western Narrative of HealingДокумент87 страницCombining Stories: Reading Tibetan Medicine As A Western Narrative of HealingDevin Gonier100% (1)
- Traditional HealingДокумент14 страницTraditional Healingdocuments2020Оценок пока нет
- The Revised Intrinsic/Extrinsic Religious Orientation Scale in A Sample of Attica's InhabitantsДокумент12 страницThe Revised Intrinsic/Extrinsic Religious Orientation Scale in A Sample of Attica's InhabitantslathОценок пока нет
- Religious Values in Clinical Practice Are Here To StayДокумент7 страницReligious Values in Clinical Practice Are Here To StayTibor GalacziОценок пока нет
- Ray-Wyatt2018 Article ReligionAndSpiritualityAsACultДокумент12 страницRay-Wyatt2018 Article ReligionAndSpiritualityAsACultJoe PresleyОценок пока нет
- Esoteric HealingДокумент12 страницEsoteric HealingWitchtopia Realm100% (5)
- Worldviews That Relate Humanity To Spirituality And, Sometimes, ToДокумент4 страницыWorldviews That Relate Humanity To Spirituality And, Sometimes, ToRichdarlan CalvarioОценок пока нет
- Ps111 Spirituality 2010 eДокумент4 страницыPs111 Spirituality 2010 enersitiulfahОценок пока нет
- Mark Lyons 2010Документ11 страницMark Lyons 2010Drosler MedqsОценок пока нет
- Cadge - Spiritual Assessment Tools in HealthcareДокумент8 страницCadge - Spiritual Assessment Tools in Healthcaremasmicko07Оценок пока нет
- Religious Attributions Pertaining To The Causes and Cures of Mental IllnessДокумент15 страницReligious Attributions Pertaining To The Causes and Cures of Mental IllnessDayana RomeroОценок пока нет
- Pain and Suffering As Viewed by The Hindu Religion: Ocus RticleДокумент7 страницPain and Suffering As Viewed by The Hindu Religion: Ocus RticlekavithaОценок пока нет
- Pain and Suffering As Viewed by The Hindu Religion: Ocus RticleДокумент7 страницPain and Suffering As Viewed by The Hindu Religion: Ocus RticleszОценок пока нет
- Medicine - Religion - Spirituality: Global Perspectives on Traditional, Complementary, and Alternative HealingОт EverandMedicine - Religion - Spirituality: Global Perspectives on Traditional, Complementary, and Alternative HealingDorothea LüddeckensОценок пока нет
- JurnalДокумент21 страницаJurnalyesi martinaОценок пока нет
- Resort To Faith Healing Practices in The Pathway To Care For Mental Illness A Study On Psychiatric Inpatients in OrissaДокумент13 страницResort To Faith Healing Practices in The Pathway To Care For Mental Illness A Study On Psychiatric Inpatients in OrissaGuilherme Alves PereiraОценок пока нет
- Albuquerque 2018Документ13 страницAlbuquerque 2018ANA VLADIA FERREIRA DE FREITASОценок пока нет
- Research Philo of Religion by Kenneth Ekene OnwusakaДокумент15 страницResearch Philo of Religion by Kenneth Ekene OnwusakaKenneth OnwusakaОценок пока нет
- Flourishing: Health, Disease, and Bioethics in Theological PerspectiveОт EverandFlourishing: Health, Disease, and Bioethics in Theological PerspectiveОценок пока нет
- Spiritual CareДокумент7 страницSpiritual CareSyarief NurseОценок пока нет
- Religion & Spirituality in MHДокумент18 страницReligion & Spirituality in MHspurthi_16Оценок пока нет
- Oct 28 Psychology of Religious Healing Ethical ImplicationsДокумент19 страницOct 28 Psychology of Religious Healing Ethical ImplicationsChau Minh TrietОценок пока нет
- Olivia Mam Movie AnalysisДокумент21 страницаOlivia Mam Movie AnalysisVasundhara RanaОценок пока нет
- Alternative Therapies Social History enДокумент10 страницAlternative Therapies Social History enjfjjfjfjjfjfОценок пока нет
- Folk Wisdom and Traditional Healing PracticesДокумент21 страницаFolk Wisdom and Traditional Healing Practicesnishita.sОценок пока нет
- Lysander Nesamoni 198909 MPhilF Thesis PDFДокумент137 страницLysander Nesamoni 198909 MPhilF Thesis PDFAnjani KumarОценок пока нет
- Spiritual Care in NursingДокумент5 страницSpiritual Care in NursingJose Vicente A. FaderonОценок пока нет
- Culturally Competent Care at The End of Life: A Hindu PerspectiveДокумент12 страницCulturally Competent Care at The End of Life: A Hindu PerspectiveAn YênОценок пока нет
- Espiritual y Rehabilitacion KarinДокумент8 страницEspiritual y Rehabilitacion KarinBeatriz Helena GomezОценок пока нет
- Longing For Health A Practice of Religious HealingДокумент12 страницLonging For Health A Practice of Religious HealingDanielОценок пока нет
- Religion, Spirituality, and The Practice of Medicine: Timothy P. Daaleman, DOДокумент7 страницReligion, Spirituality, and The Practice of Medicine: Timothy P. Daaleman, DOJoe PresleyОценок пока нет
- BaixaДокумент7 страницBaixaXavi Alsina CaulasОценок пока нет
- AMA Journal of Ethics: July 2018, Volume 20, Number 7: E655-663Документ9 страницAMA Journal of Ethics: July 2018, Volume 20, Number 7: E655-663Eva Garcia MartinezОценок пока нет
- Spirituality and Healing - Torosian 2005Документ5 страницSpirituality and Healing - Torosian 2005Mércia FiuzaОценок пока нет
- Introduction To The Special Issue On Spirituality and PsychotheraДокумент6 страницIntroduction To The Special Issue On Spirituality and PsychotheraAlena ShakhovaОценок пока нет
- Bioethics and TheologyДокумент5 страницBioethics and TheologyfaiqausmanОценок пока нет
- Chinese Patients' Perceptions of Health, IllnessДокумент8 страницChinese Patients' Perceptions of Health, IllnessclОценок пока нет
- Interventions To Enhance The Spiritual Aspects of Dying: Journal of Palliative Medicine February 2005Документ15 страницInterventions To Enhance The Spiritual Aspects of Dying: Journal of Palliative Medicine February 2005Liana Pérez RodríguezОценок пока нет
- 69443164Документ78 страниц69443164Kenn yahweexОценок пока нет
- Freshmen Students Bank Procedures For Non-ATM Accounts or CashДокумент2 страницыFreshmen Students Bank Procedures For Non-ATM Accounts or CashKenn yahweexОценок пока нет
- Tinetti PDFДокумент2 страницыTinetti PDFKenn yahweexОценок пока нет
- Critical Care Notes Clinical Pocket Guide - (Gastro-Urinary)Документ1 страницаCritical Care Notes Clinical Pocket Guide - (Gastro-Urinary)Britanny Nelson100% (1)
- Pancreatic Cancer 1-ACS-tugas DR TeharДокумент63 страницыPancreatic Cancer 1-ACS-tugas DR Teharalyssafairudz21Оценок пока нет
- Nclex-Gi 2Документ1 страницаNclex-Gi 2Kenn yahweexОценок пока нет
- DNJKFNKDNKLFДокумент2 страницыDNJKFNKDNKLFKenn yahweexОценок пока нет
- International LawДокумент13 страницInternational LawKenn yahweexОценок пока нет
- Journal DR RequirementДокумент10 страницJournal DR RequirementKenn yahweexОценок пока нет
- Journal Ortho RequirementДокумент13 страницJournal Ortho RequirementKenn yahweexОценок пока нет
- THRAДокумент8 страницTHRAKenn yahweexОценок пока нет
- Journal Ortho RequirementДокумент13 страницJournal Ortho RequirementKenn yahweexОценок пока нет
- GDS Scale PDFДокумент2 страницыGDS Scale PDFDiyah RahmawatiОценок пока нет
- Pneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaДокумент7 страницPneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaKenn yahweexОценок пока нет
- NCPДокумент6 страницNCPKenn yahweexОценок пока нет
- Online EnrollДокумент19 страницOnline EnrollKenn yahweexОценок пока нет
- Communicablediseaseqa 140829080936 Phpapp02Документ20 страницCommunicablediseaseqa 140829080936 Phpapp02Keiarah Kath Estrada CallaoОценок пока нет
- Reported Pain Scale of 5/10 Being 10 As The Most Painful Score at The Surgical Site Descibed As Dull PainДокумент1 страницаReported Pain Scale of 5/10 Being 10 As The Most Painful Score at The Surgical Site Descibed As Dull PainKenn yahweexОценок пока нет
- Drug StudyДокумент11 страницDrug StudyKenn yahweexОценок пока нет
- DOHStat Health Status-MortalityДокумент25 страницDOHStat Health Status-MortalityKenn yahweexОценок пока нет
- CHN RXN PaperДокумент1 страницаCHN RXN PaperKenn yahweexОценок пока нет
- Cavendish 2004Документ18 страницCavendish 2004Kenn yahweexОценок пока нет
- Ascending Polyneuropathic Paralysis) Is An Acute, Rapidly Progressing, and Potentially Fatal Form ofДокумент8 страницAscending Polyneuropathic Paralysis) Is An Acute, Rapidly Progressing, and Potentially Fatal Form ofKenn yahweexОценок пока нет
- Integrating Spirituality Into Nurse Practitioner Practice:: The Importance of Finding The TimeДокумент8 страницIntegrating Spirituality Into Nurse Practitioner Practice:: The Importance of Finding The TimeKenn yahweexОценок пока нет
- IntroductionДокумент12 страницIntroductionKenn yahweexОценок пока нет
- The Dying Process Death Is Defined AsДокумент5 страницThe Dying Process Death Is Defined AsKenn yahweexОценок пока нет
- Structure and Function of The Skeletal System: Skeleton Dried Up BodyДокумент4 страницыStructure and Function of The Skeletal System: Skeleton Dried Up BodyKenn yahweexОценок пока нет
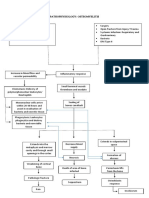
- PathophysiologyДокумент2 страницыPathophysiologyKenn yahweexОценок пока нет
- Patient's ProfileДокумент1 страницаPatient's ProfileKenn yahweexОценок пока нет
- OsteomyelitisДокумент7 страницOsteomyelitisKenn yahweexОценок пока нет
- Midwife in AustraliaДокумент13 страницMidwife in AustraliaNinne GerdhaОценок пока нет
- Anthony Filly CVДокумент5 страницAnthony Filly CVapi-289727140Оценок пока нет
- Family-Centred Practice: Empowerment, Self-Efficacy, and Challenges For Practitioners in Early Childhood Education and CareДокумент11 страницFamily-Centred Practice: Empowerment, Self-Efficacy, and Challenges For Practitioners in Early Childhood Education and CareciaoОценок пока нет
- Mspe RecommendationДокумент11 страницMspe RecommendationJuanОценок пока нет
- The All India Services (Med Att Rules) - Misc InstructionsДокумент22 страницыThe All India Services (Med Att Rules) - Misc InstructionsJitendra Suraaj TripathiОценок пока нет
- DD Form 31Документ5 страницDD Form 31Aaron HaganОценок пока нет
- Nurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesДокумент10 страницNurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesLesterОценок пока нет
- Foundation Course MBBS PDFДокумент10 страницFoundation Course MBBS PDFVirendra Kumar GajbhiyeОценок пока нет
- Chapter 2. Integrating Risk Management, Quality, Management, and Patient SafetyДокумент10 страницChapter 2. Integrating Risk Management, Quality, Management, and Patient SafetyNi Putu Sri wahyuniОценок пока нет
- Kothala HimbutuДокумент2 страницыKothala HimbutuHashan ErandaОценок пока нет
- Oxygen Therapies: Interview With Ed MccabeДокумент5 страницOxygen Therapies: Interview With Ed MccabeOrlando Gunther100% (1)
- Career Research Paper On Registered NurseДокумент6 страницCareer Research Paper On Registered Nurseh03318kj100% (1)
- SáchДокумент52 страницыSáchVõ Văn Phúc ToànОценок пока нет
- Medical Form DoleДокумент8 страницMedical Form DolejaysonmalaaОценок пока нет
- Ozone TherapyДокумент24 страницыOzone TherapyDadoBabylobas100% (2)
- Elkefi Et Al 2022 Impact of Health Informatics On Patients Perception of Health Care Services Trends Over Time ofДокумент6 страницElkefi Et Al 2022 Impact of Health Informatics On Patients Perception of Health Care Services Trends Over Time ofeva kacanjaОценок пока нет
- Access, Cost, and Quality For APNsДокумент6 страницAccess, Cost, and Quality For APNsMellyne SallyОценок пока нет
- Duties and Responsibilities of Chief Medical OfficerДокумент18 страницDuties and Responsibilities of Chief Medical OfficerkgnmatinОценок пока нет
- Residency Prog CanadaДокумент116 страницResidency Prog Canadahswami20037730Оценок пока нет
- Etika Kedokteran: Dan ProfesionalismeДокумент39 страницEtika Kedokteran: Dan ProfesionalismeNandaОценок пока нет
- Traditional Chinese Medicine PDFДокумент32 страницыTraditional Chinese Medicine PDFGg KОценок пока нет
- Taxation Law FD (Saurav) Word FileДокумент15 страницTaxation Law FD (Saurav) Word Filesaurav singh100% (1)
- Shelley Anandhavalli. EДокумент15 страницShelley Anandhavalli. EPrisha BauskarОценок пока нет
- EMS Agenda For The FutureДокумент106 страницEMS Agenda For The FutureepraetorianОценок пока нет
- Gloria M. Dela Cruz: Personal DataДокумент4 страницыGloria M. Dela Cruz: Personal Datamissglorya100% (1)
- The Impact of Using The Information Technology On The Quality of Health Services in The Hospitals of Private Sector in NajranДокумент12 страницThe Impact of Using The Information Technology On The Quality of Health Services in The Hospitals of Private Sector in NajraninventionjournalsОценок пока нет
- Annotated Bibliography FinalДокумент3 страницыAnnotated Bibliography Finalapi-263873257Оценок пока нет
- Running Head: Iturralde V. Hilo Medical Center Usa: Case Study 1Документ11 страницRunning Head: Iturralde V. Hilo Medical Center Usa: Case Study 1HugsОценок пока нет
- Mistymcdowellweek 13 PublishresumeДокумент9 страницMistymcdowellweek 13 Publishresumeapi-427353740Оценок пока нет
- Pharmacognosy Stdy of CT MTTДокумент188 страницPharmacognosy Stdy of CT MTTsairabatoolОценок пока нет