Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- QuistionareeeДокумент7 страницQuistionareeenilamОценок пока нет
- Narrator: Oulyvia MaritaДокумент2 страницыNarrator: Oulyvia MaritanilamОценок пока нет
- American Journal of Infection Control: Major ArticleДокумент7 страницAmerican Journal of Infection Control: Major ArticlenilamОценок пока нет
- The Incidence and Risk of Infusion Phlebitis With Peripheral Intravenous Catheters: A Meta-AnalysisДокумент8 страницThe Incidence and Risk of Infusion Phlebitis With Peripheral Intravenous Catheters: A Meta-AnalysisnilamОценок пока нет
- Appraisal Analysis of "U-23 Coach Says Ready To Take Responsibility If Match-Fixing Allegation True" NewsДокумент8 страницAppraisal Analysis of "U-23 Coach Says Ready To Take Responsibility If Match-Fixing Allegation True" NewsnilamОценок пока нет
- Avina & Drones Lyrics: "Glass Bridge"Документ1 страницаAvina & Drones Lyrics: "Glass Bridge"nilamОценок пока нет
- Spring Fling: CelebrationДокумент1 страницаSpring Fling: CelebrationnilamОценок пока нет
- Kekerasan Dalam Rumah Tangga Dilihat Dari Aspek Viktimologi Dan Hukum PidanaДокумент21 страницаKekerasan Dalam Rumah Tangga Dilihat Dari Aspek Viktimologi Dan Hukum PidananilamОценок пока нет
- The Nature of Spiritual Hunger: Oyewole O. Sarumi - PHDДокумент37 страницThe Nature of Spiritual Hunger: Oyewole O. Sarumi - PHDnilamОценок пока нет
- Demi Lovato LyricДокумент4 страницыDemi Lovato LyricnilamОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Susunan Acara Pelatihan BTCLS RS Graha Hermine BatamДокумент4 страницыSusunan Acara Pelatihan BTCLS RS Graha Hermine BatamDina MariyanaОценок пока нет
- Edexcel GCSE P.E. (Physical Education) Revision Guide & Workbook SampleДокумент12 страницEdexcel GCSE P.E. (Physical Education) Revision Guide & Workbook SamplePearson Schools100% (3)
- 007 - Cardiovascular Physiology) MASTER ECGДокумент8 страниц007 - Cardiovascular Physiology) MASTER ECGSWATHIKA L100% (1)
- Dealing With Familiar SpiritsДокумент7 страницDealing With Familiar Spiritsvictor mogajaneОценок пока нет
- 100 ECG For AKP - With AnswersДокумент102 страницы100 ECG For AKP - With AnswersaeyousefОценок пока нет
- The Thoracic CavityДокумент2 страницыThe Thoracic CavityApril MarieОценок пока нет
- Sotry Board Dan ScriptДокумент4 страницыSotry Board Dan Scriptnuex01Оценок пока нет
- (Pulse of Heart and Brain) Analysis Report Card: Actual Testing ResultsДокумент2 страницы(Pulse of Heart and Brain) Analysis Report Card: Actual Testing ResultsanuОценок пока нет
- Harvey ManualДокумент89 страницHarvey ManualFlowerОценок пока нет
- College of Nursing: Pharmacological ManagementДокумент4 страницыCollege of Nursing: Pharmacological ManagementBianca Mikaela DosdosОценок пока нет
- Heart Disease in Malaysia (2014) : Puteri Syazreen Athillah Nabilah HamidДокумент2 страницыHeart Disease in Malaysia (2014) : Puteri Syazreen Athillah Nabilah HamidCIK FATHINОценок пока нет
- Grade 6 2nd Periodical Test With TOS & Answer Keys SCIENCEДокумент10 страницGrade 6 2nd Periodical Test With TOS & Answer Keys SCIENCEPaulo MarianoОценок пока нет
- 6BI05 01 Que 20150617Документ24 страницы6BI05 01 Que 20150617Ammar ZavahirОценок пока нет
- Paag Esc Congress 2021Документ14 страницPaag Esc Congress 2021Carlos MlОценок пока нет
- Common Valvular Heart Disease (At A Glance)Документ1 страницаCommon Valvular Heart Disease (At A Glance)Tamim IshtiaqueОценок пока нет
- AQA A Level Biology Unit 1 NotesДокумент17 страницAQA A Level Biology Unit 1 NotesMuadh Chati100% (3)
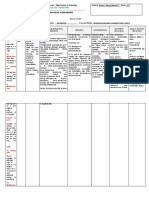
- Nursing Care Plan Cues Nursing Diagnosis Objectives Intervention Rationale EvaluationДокумент10 страницNursing Care Plan Cues Nursing Diagnosis Objectives Intervention Rationale EvaluationMargareth GonzalesОценок пока нет
- SNC2D1 Biology Unit ReviewДокумент3 страницыSNC2D1 Biology Unit ReviewSA - 10WB 933839 The Woodlands SSОценок пока нет
- Sahya Part 4Документ116 страницSahya Part 4Homeopathy Torrents100% (1)
- Low Cardiac Output SyndromeДокумент21 страницаLow Cardiac Output SyndromeMuaath Algoribi100% (1)
- Amy Jo Ellis Enhancing Your Life Using The Court of AtonementДокумент30 страницAmy Jo Ellis Enhancing Your Life Using The Court of AtonementJohnny Konstantinou100% (2)
- Critical Care Nursing Notes 1Документ10 страницCritical Care Nursing Notes 1pauchanmnlОценок пока нет
- NCMB 312 - MS1 Course Task Cu1Документ3 страницыNCMB 312 - MS1 Course Task Cu1HeinzzzОценок пока нет
- 1 Evaluation and Management of ShockДокумент11 страниц1 Evaluation and Management of ShockYESSICA CARENALGAОценок пока нет
- Physiotherapy Guideline: Queensland Cardiorespiratory Physiotherapy NetworkДокумент20 страницPhysiotherapy Guideline: Queensland Cardiorespiratory Physiotherapy NetworkBRDОценок пока нет
- MCN Lec Practice QuestionsДокумент14 страницMCN Lec Practice QuestionsTrishaОценок пока нет
- Vijay ShreeДокумент98 страницVijay ShreeRafi SungkarОценок пока нет
- Science 4 Lesson PlanДокумент11 страницScience 4 Lesson PlanEmily BucsitОценок пока нет
- EcgДокумент86 страницEcgHidayatul ゆきОценок пока нет
- Study-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsДокумент17 страницStudy-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsDan Dan ManaoisОценок пока нет