Вам также может понравиться
- HIV Statistical Report 2011Документ13 страницHIV Statistical Report 2011Franklin MartinezОценок пока нет
- Profile of Chickenpox Cases in J.N. Institute of Medical Sciences, Imphal: A Descriptive StudyДокумент3 страницыProfile of Chickenpox Cases in J.N. Institute of Medical Sciences, Imphal: A Descriptive StudySyaika Amelia ZahraОценок пока нет
- Ministry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Документ13 страницMinistry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Hussein H. MahmoodОценок пока нет
- HIV Infection: What Should We Know?: Ridwan BalatifДокумент16 страницHIV Infection: What Should We Know?: Ridwan BalatifSri AnggrianiОценок пока нет
- Oregon Health Authority COVID-19 Weekly Report (Published 10/28)Документ38 страницOregon Health Authority COVID-19 Weekly Report (Published 10/28)KGW NewsОценок пока нет
- Him Exercise Group 4Документ8 страницHim Exercise Group 4Sarrie MunkutikeОценок пока нет
- Health Notions, Volume 3 Number 7 (July 2019) Issn 2580-4936Документ4 страницыHealth Notions, Volume 3 Number 7 (July 2019) Issn 2580-4936Siti rohmatul LailyОценок пока нет
- Oregon COVID-19 Weekly Report (Published Oct. 21, 2020)Документ33 страницыOregon COVID-19 Weekly Report (Published Oct. 21, 2020)KGW NewsОценок пока нет
- Sti/StdДокумент34 страницыSti/Stdtsega tilahunОценок пока нет
- Covid 19 Weekly Report 2020-11-18 FinalДокумент50 страницCovid 19 Weekly Report 2020-11-18 FinalSinclair Broadcast Group - EugeneОценок пока нет
- HIV in Colombia: An Epidemiologic Point of ViewДокумент8 страницHIV in Colombia: An Epidemiologic Point of ViewJuanJoseHerreraBerrioОценок пока нет
- Background: Measles Is A Highly Contagious Disease Caused by Viruses That CanДокумент7 страницBackground: Measles Is A Highly Contagious Disease Caused by Viruses That CanWardiansyah NaimОценок пока нет
- Oregon Health Authority COVID-19 Weekly Report (Published 10/7)Документ31 страницаOregon Health Authority COVID-19 Weekly Report (Published 10/7)KGW NewsОценок пока нет
- Jurnal CovidДокумент4 страницыJurnal CovidSarce CheОценок пока нет
- Shuyihoo Excelassignment Chlamydia FinalДокумент80 страницShuyihoo Excelassignment Chlamydia Finalapi-236381148Оценок пока нет
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1От EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Оценок пока нет
- Art08 1Документ7 страницArt08 1andrea andradeОценок пока нет
- Descriptive EpidemiologyДокумент23 страницыDescriptive EpidemiologyHari SaduОценок пока нет
- UDOH COVID-19 Brief June 19Документ8 страницUDOH COVID-19 Brief June 19LarryDCurtis100% (1)
- A Systematic Review and Meta Analysis of Children With Coronavirus Disease 2019 (COVID 19)Документ13 страницA Systematic Review and Meta Analysis of Children With Coronavirus Disease 2019 (COVID 19)Jevera JoshuaОценок пока нет
- Effects of Response To 2014-2015 Ebola Outbreak On Deaths From Malaria, HIV/AIDS, and Tuberculosis, West AfricaДокумент9 страницEffects of Response To 2014-2015 Ebola Outbreak On Deaths From Malaria, HIV/AIDS, and Tuberculosis, West AfricaIka tenri saliОценок пока нет
- CDC 99478 DS1Документ4 страницыCDC 99478 DS1Leandro CesarОценок пока нет
- 2018 HIV STD OverviewДокумент40 страниц2018 HIV STD OverviewMadeline CiakОценок пока нет
- 4MMWR-Severe Outcomes Among Patients With Coronavirus Disease 2019 COVID-19-United States February 12-March 16 2020 PDFДокумент4 страницы4MMWR-Severe Outcomes Among Patients With Coronavirus Disease 2019 COVID-19-United States February 12-March 16 2020 PDFCarlos Alberto Hernandez TorresОценок пока нет
- Infectious and Congenital Syphilis in Canada, 2010-2015: Y Choudhri, J Miller, J Sandhu, A Leon, J AhoДокумент6 страницInfectious and Congenital Syphilis in Canada, 2010-2015: Y Choudhri, J Miller, J Sandhu, A Leon, J AhoKrinta AlisaОценок пока нет
- Lung Cancer Peru 2020Документ8 страницLung Cancer Peru 2020Anthony Jason Castro JustinianoОценок пока нет
- A Practical Approach To The Diagnosis and Treatment of Vitiligo in Children PDFДокумент14 страницA Practical Approach To The Diagnosis and Treatment of Vitiligo in Children PDFsriworoОценок пока нет
- BPJ - SPL - Edn. 1 - P - 25-30Документ6 страницBPJ - SPL - Edn. 1 - P - 25-30andre redobleОценок пока нет
- Oregon COVID-19 Weekly Report (Published Dec. 16)Документ16 страницOregon COVID-19 Weekly Report (Published Dec. 16)KGW NewsОценок пока нет
- St. Louis County Health Department COVID-19 Report For Sept. 2, 2021Документ24 страницыSt. Louis County Health Department COVID-19 Report For Sept. 2, 2021KSDKОценок пока нет
- Journal SiflisДокумент10 страницJournal SiflisElang SudewaОценок пока нет
- 1level of Underreporting Including Underdiagnosis Before The First Peak of Covid19 in Various Countries Preliminary Retrospective Results Based On Wavelets and Deterministic ModelingДокумент3 страницы1level of Underreporting Including Underdiagnosis Before The First Peak of Covid19 in Various Countries Preliminary Retrospective Results Based On Wavelets and Deterministic ModelingEduardo Jose Caicedo GomezОценок пока нет
- Medicina TropicalДокумент9 страницMedicina TropicalSamuel ChavesОценок пока нет
- Epidemiological Survey On Cutaneous Leishmaniasis in A Rural Area at Baghdad-Iraq 2020Документ3 страницыEpidemiological Survey On Cutaneous Leishmaniasis in A Rural Area at Baghdad-Iraq 2020International Journal of Innovative Science and Research TechnologyОценок пока нет
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterДокумент4 страницыNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterJohn RoxasОценок пока нет
- Increase in Measles Cases - United States, January 1-April 26, 2019Документ3 страницыIncrease in Measles Cases - United States, January 1-April 26, 2019inforumdocsОценок пока нет
- Telaah Kritis JurnalДокумент8 страницTelaah Kritis JurnalZIDNASABELANОценок пока нет
- Clinical Epidemiological Profile of Vitiligo in Children and AdolescentsДокумент3 страницыClinical Epidemiological Profile of Vitiligo in Children and AdolescentsKarla KaluaОценок пока нет
- Covid ReportДокумент20 страницCovid ReportMarianne MartinezОценок пока нет
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterДокумент4 страницыNewly Diagnosed HIV Cases in The Philippines: National Epidemiology Centerkornets1220Оценок пока нет
- Surveillance For Lyme Disease After Implementation of A Revised Case Definition - United States, 2022Документ21 страницаSurveillance For Lyme Disease After Implementation of A Revised Case Definition - United States, 2022worksheetbookОценок пока нет
- Final Version of HIV ResearchДокумент29 страницFinal Version of HIV ResearchJordan Abosama MamalumpongОценок пока нет
- DocxДокумент4 страницыDocxFarah FarahОценок пока нет
- Travel Medicine and Infectious Disease: CorrespondenceДокумент3 страницыTravel Medicine and Infectious Disease: CorrespondenceanomОценок пока нет
- April 29 UP OCTA Research Covid 19 in The Philippines Forecast Report No.5 - EaaДокумент15 страницApril 29 UP OCTA Research Covid 19 in The Philippines Forecast Report No.5 - EaaJessa Bienel Biagtas OlescoОценок пока нет
- 4 IndonesiaДокумент12 страниц4 IndonesiaGyanNurmaindahHendiantiОценок пока нет
- Coping and Health in Tanzania (CHAT) : Preliminary FindingsДокумент27 страницCoping and Health in Tanzania (CHAT) : Preliminary Findingskyle_hamilton9947Оценок пока нет
- Articulo 4Документ5 страницArticulo 4Daniella Rodriguez ReyesОценок пока нет
- Oregon Health Authority COVID-19 Weekly Report (Published Nov. 12)Документ45 страницOregon Health Authority COVID-19 Weekly Report (Published Nov. 12)KGW NewsОценок пока нет
- Review Article Leprosy: A Review of Epidemiology, Clinical Diagnosis, and ManagementДокумент13 страницReview Article Leprosy: A Review of Epidemiology, Clinical Diagnosis, and ManagementeugeniaОценок пока нет
- COVID-19 - Evidence Over Hysteria - Zero HedgeДокумент38 страницCOVID-19 - Evidence Over Hysteria - Zero HedgeFabiana BОценок пока нет
- Science Abc3517 FullДокумент9 страницScience Abc3517 FullroopОценок пока нет
- Morb, F1+, MortNat, A1Prog, Demo, M2, A1 Program FormsДокумент30 страницMorb, F1+, MortNat, A1Prog, Demo, M2, A1 Program FormsReuben Jr UmallaОценок пока нет
- Jurnal 5 TridaraДокумент5 страницJurnal 5 TridaraLuckyNawaОценок пока нет
- Situasi DBD Di Indonesia. Pusat Data Dan Informasi Kementrian Kesehatan RI.2016Документ6 страницSituasi DBD Di Indonesia. Pusat Data Dan Informasi Kementrian Kesehatan RI.2016El Alsha AndiniОценок пока нет
- TB Vih JaponДокумент8 страницTB Vih JaponLuis LeccaОценок пока нет
- GISP Supplement AggrFigs AggrTables Clinic Profiles 2015Документ284 страницыGISP Supplement AggrFigs AggrTables Clinic Profiles 2015Ruth López BarrachinaОценок пока нет
- Acne Relapses Impact On Quality of Life and Productivity2019Документ7 страницAcne Relapses Impact On Quality of Life and Productivity2019sara3elena3manolacheОценок пока нет
- The War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersОт EverandThe War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersОценок пока нет
- Filed Complaint Er v. MT Carmel - Filed ComplaintДокумент11 страницFiled Complaint Er v. MT Carmel - Filed ComplaintSam Winstrom100% (1)
- Nyx Lieutenants Response To AttorneyДокумент2 страницыNyx Lieutenants Response To AttorneySam WinstromОценок пока нет
- Nyx LetterДокумент1 страницаNyx LetterSam WinstromОценок пока нет
- Tre'Mall McGee ComplaintДокумент36 страницTre'Mall McGee ComplaintSam WinstromОценок пока нет
- JPSS Reported Fights and ConsequencesДокумент5 страницJPSS Reported Fights and ConsequencesSam WinstromОценок пока нет
- Chris Roberts IndictmentДокумент32 страницыChris Roberts IndictmentSam Winstrom100% (1)
- AG March 24 2019 Letter To House and Senate Judiciary CommitteesДокумент4 страницыAG March 24 2019 Letter To House and Senate Judiciary Committeesblc8893% (70)
- Fennidy vs. Christ The King Parish SchoolДокумент10 страницFennidy vs. Christ The King Parish SchoolSam WinstromОценок пока нет
- Class Action Lawsuit Against Make It Right FoundationДокумент30 страницClass Action Lawsuit Against Make It Right FoundationSam WinstromОценок пока нет
- Sharon Lo Drucker Police ReportДокумент7 страницSharon Lo Drucker Police ReportSam WinstromОценок пока нет
- Jacob Johnson vs. Daryl PurperaДокумент9 страницJacob Johnson vs. Daryl PurperaSam WinstromОценок пока нет
- Louisiana Board of Pharmacy Guidelines On CBD OilДокумент2 страницыLouisiana Board of Pharmacy Guidelines On CBD OilSam WinstromОценок пока нет
- Drainage ReportДокумент18 страницDrainage ReportSam WinstromОценок пока нет
- AG Landry Has Given Out More Than 100 'Honorary Badges' Since He Took OfficeДокумент1 страницаAG Landry Has Given Out More Than 100 'Honorary Badges' Since He Took OfficeSam WinstromОценок пока нет
- Cedric Grant Requests FEMA Redirect $35 Million To S&WB ProjectsДокумент1 страницаCedric Grant Requests FEMA Redirect $35 Million To S&WB ProjectsSam WinstromОценок пока нет
- Alton Sterling Autopsy ReportДокумент9 страницAlton Sterling Autopsy ReportSam WinstromОценок пока нет
- Jazz Fest Cubes 2018Документ7 страницJazz Fest Cubes 2018Sam WinstromОценок пока нет
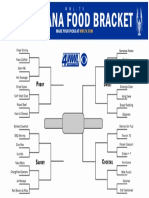
- Louisiana Food BracketДокумент1 страницаLouisiana Food BracketSam Winstrom80% (5)
- HEAL Audit SummaryДокумент1 страницаHEAL Audit SummarySam WinstromОценок пока нет
- Jefferson Parish Finance Authority Public Audit ReportДокумент304 страницыJefferson Parish Finance Authority Public Audit ReportSam WinstromОценок пока нет
- DepEd WiNS Program ValidationДокумент36 страницDepEd WiNS Program ValidationJANETH POLINAR100% (1)
- 1 3 19 668 PDFДокумент2 страницы1 3 19 668 PDFLetsShop BbsrОценок пока нет
- Managing Workplace Safety and HealthДокумент15 страницManaging Workplace Safety and HealthnitinmtОценок пока нет
- Communicable Disease NursingДокумент9 страницCommunicable Disease NursingMaybelyn JoradoОценок пока нет
- Calawis Water Treatment PlantДокумент4 страницыCalawis Water Treatment PlantSakura ShigaОценок пока нет
- Sanitation Saftey Midterm 2021Документ5 страницSanitation Saftey Midterm 2021Jah BinksОценок пока нет
- Brunette Eloise A. Cesa - April 15, 2022Документ12 страницBrunette Eloise A. Cesa - April 15, 2022Jackielou MaquisoОценок пока нет
- Gastroenteritis: Escherichia ColiДокумент4 страницыGastroenteritis: Escherichia ColiFanny BudimanОценок пока нет
- Clinic - Rules - Extension 6Документ2 страницыClinic - Rules - Extension 6Tony LeMesmerОценок пока нет
- Tuesday, June 08, 2015 EditionДокумент18 страницTuesday, June 08, 2015 EditionFrontPageAfricaОценок пока нет
- Felocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Документ1 страницаFelocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Reginaldo ParcianelloОценок пока нет
- Potenciano A. Abejero Elementary SchoolДокумент2 страницыPotenciano A. Abejero Elementary SchoolCarlota Tejero100% (11)
- International General Certificate: Reference Information Provided, in Particular Web Links, Was Correct As of 03/04/17Документ23 страницыInternational General Certificate: Reference Information Provided, in Particular Web Links, Was Correct As of 03/04/17Satyadip TeraiyaОценок пока нет
- Elective 2 Lecture 1 Concept of IllnessДокумент9 страницElective 2 Lecture 1 Concept of IllnessMelchor Felipe Salvosa100% (1)
- Brand Training Midcon v4 SM Material 1 1Документ88 страницBrand Training Midcon v4 SM Material 1 1Jenny FerОценок пока нет
- Stages of HivДокумент4 страницыStages of Hivapi-273431943Оценок пока нет
- CPH PrefinalДокумент22 страницыCPH PrefinalZharmaine ChavezОценок пока нет
- Biosafety Levels: Primary ContainmentДокумент8 страницBiosafety Levels: Primary ContainmentAbeer FatimaОценок пока нет
- Ejaib42020 PDFДокумент64 страницыEjaib42020 PDFAngelica ConvocarОценок пока нет
- PM 286 BДокумент2 страницыPM 286 Bnasreen95035Оценок пока нет
- Management of Breast FeedingДокумент17 страницManagement of Breast FeedingUday KumarОценок пока нет
- PDF 2420872588Документ1 страницаPDF 2420872588kariem noweerОценок пока нет
- Swine Flu WhitepaperДокумент95 страницSwine Flu WhitepaperPatrick Savalle100% (1)
- TPDES Permit Issuance Request LetterДокумент6 страницTPDES Permit Issuance Request LetterKUTNewsОценок пока нет
- Notice: Committees Establishment, Renewal, Termination, Etc.: Physical Activity Guidelines Advisory CommitteeДокумент2 страницыNotice: Committees Establishment, Renewal, Termination, Etc.: Physical Activity Guidelines Advisory CommitteeJustia.comОценок пока нет
- Tips For A Healthy PregnancyДокумент2 страницыTips For A Healthy PregnancyLizaОценок пока нет
- Nutrition Services Screening Assessment (NSSA) SebagaiДокумент8 страницNutrition Services Screening Assessment (NSSA) SebagaiEko RistiyantoОценок пока нет
- Executive Assistant Job DescriptionДокумент2 страницыExecutive Assistant Job DescriptionColumbia SSRSОценок пока нет
- Barangay Pulo: Republic of The Philippines City of ValenzuelaДокумент3 страницыBarangay Pulo: Republic of The Philippines City of ValenzuelaBarangay Pulo ValenzuelaОценок пока нет
- Tutorial Group 1Документ6 страницTutorial Group 1Sanjeev NehruОценок пока нет