Вам также может понравиться
- EmpyemaДокумент17 страницEmpyemadeo_gratias14Оценок пока нет
- Senam LafiskaДокумент6 страницSenam LafiskaAyuОценок пока нет
- Algoritma TBIДокумент3 страницыAlgoritma TBIravenskaОценок пока нет
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisОт EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Anatomi Telinga & Fisiologi PendengaranДокумент5 страницAnatomi Telinga & Fisiologi PendengaranjuliperОценок пока нет
- Gagal NafasДокумент33 страницыGagal NafastitoОценок пока нет
- WOC Bronkitis AkutДокумент1 страницаWOC Bronkitis AkutkurniaОценок пока нет
- Emailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFДокумент38 страницEmailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFHaykal FathirrahmanОценок пока нет
- Edema ParuДокумент42 страницыEdema ParuGP RS EMCОценок пока нет
- Jadwal DokterДокумент1 страницаJadwal DokterHuda ZiyadОценок пока нет
- A. WOC Acute Lungs Oedem.: Gangguan Perfusi JaringanДокумент1 страницаA. WOC Acute Lungs Oedem.: Gangguan Perfusi Jaringanrizki vitaОценок пока нет
- Pengaruh Pemberian Infus Hangat Terhadap Stabilitas Suhu Tubuh Pada Pasien Post Operasi General Anestesi Di Recovery Room Rsu Karsa Husada BatuДокумент7 страницPengaruh Pemberian Infus Hangat Terhadap Stabilitas Suhu Tubuh Pada Pasien Post Operasi General Anestesi Di Recovery Room Rsu Karsa Husada BatuKonsul Dosen PembibingОценок пока нет
- ENG - Hiperplasia EndometriumДокумент19 страницENG - Hiperplasia EndometriumIrwin FitriansyahОценок пока нет
- Patofisiologi Tumor KolonДокумент2 страницыPatofisiologi Tumor Kolonnur hijriahОценок пока нет
- Different Zones in OTДокумент1 страницаDifferent Zones in OTbindukrishna01Оценок пока нет
- Jumlah Tetesan Infus MakroДокумент2 страницыJumlah Tetesan Infus MakroMamanya Ef Taya ThalitaОценок пока нет
- Jurnal AMS PDFДокумент8 страницJurnal AMS PDFputriseptinaОценок пока нет
- Rangkuman ACLSДокумент13 страницRangkuman ACLSSavero Evan AbishaОценок пока нет
- SYNTHES LCP Small Fragment Instrument SetДокумент5 страницSYNTHES LCP Small Fragment Instrument SetAbdulrahmanОценок пока нет
- Jurnal AnastesiДокумент10 страницJurnal AnastesiAnonymous m07Ogz0rОценок пока нет
- Leaflet ITPДокумент2 страницыLeaflet ITPtriОценок пока нет
- Convention Modes of Mechanical Ventilation. DR - purwOKOДокумент53 страницыConvention Modes of Mechanical Ventilation. DR - purwOKOIsnia WahibОценок пока нет
- Patoflow Diagram Diabetes Mellitus Baru.1Документ2 страницыPatoflow Diagram Diabetes Mellitus Baru.1marlinОценок пока нет
- Asuhan Keperawatan Acute Respiratory Distress Syndrome (ARDS)Документ20 страницAsuhan Keperawatan Acute Respiratory Distress Syndrome (ARDS)Hendra Kurnia Rakhma100% (1)
- Kuliah Extrapyramidal SyndromeДокумент50 страницKuliah Extrapyramidal SyndromePutri Azka RinandaОценок пока нет
- Pathway Intrauterine Fetal DeathДокумент1 страницаPathway Intrauterine Fetal DeathFrengky Imanuel HermanusОценок пока нет
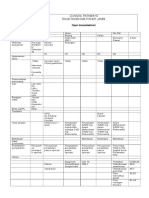
- Clinical Pathway Open CholecystektomiДокумент2 страницыClinical Pathway Open CholecystektomiAnton TrihartantoОценок пока нет
- Stroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul MulukДокумент45 страницStroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul Mulukdhea nadhiaОценок пока нет
- Askep in EnglishДокумент9 страницAskep in EnglishnoviОценок пока нет
- General AnaesthesiaДокумент53 страницыGeneral Anaesthesiapeter singal100% (2)
- Primary Survey AssessmentДокумент52 страницыPrimary Survey Assessmentlapkas donjuanОценок пока нет
- Trauma Tumpul Abdomen - Dr. Monica, SP.BДокумент54 страницыTrauma Tumpul Abdomen - Dr. Monica, SP.Brizky sitanayaОценок пока нет
- Pathway Edema ParuДокумент2 страницыPathway Edema Parunira100% (1)
- Askep AliДокумент34 страницыAskep AliadinsОценок пока нет
- Physio Ex Exercise 6 Activity 1Документ3 страницыPhysio Ex Exercise 6 Activity 1Roland Calipayan Jr.Оценок пока нет
- Referred PainДокумент1 страницаReferred PainAngelina MakinОценок пока нет
- Tehnik - Tehnik Analgesia Post OperasiДокумент32 страницыTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoОценок пока нет
- PKB Vii Papdi MakassarДокумент10 страницPKB Vii Papdi MakassarTaufik Ramadhan BiyaОценок пока нет
- Jurnal Anestesi Bahasa InggrisДокумент15 страницJurnal Anestesi Bahasa InggrisTri Utami JasmanОценок пока нет
- Leaflet Hiperplasia EndometriumДокумент2 страницыLeaflet Hiperplasia EndometriumjefryОценок пока нет
- Patofisiologi HematuriaДокумент10 страницPatofisiologi HematuriaNurunSalamanОценок пока нет
- Guideline ImphoДокумент13 страницGuideline Impho6130015051 MOHAMMAD QOIMAM BILQISTHI ZULFIKARОценок пока нет
- CVP Guided Deresuscitation in Managing Overload in Icu PDFДокумент57 страницCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- CSS Airway Management RickyДокумент53 страницыCSS Airway Management RickyArtha PutuОценок пока нет
- Monitoring Neuromuskular Kuantitatif Pada Penggunaan Muscle RelaxantДокумент17 страницMonitoring Neuromuskular Kuantitatif Pada Penggunaan Muscle RelaxantWidi Yuli HariantoОценок пока нет
- Struma Nodulus Non ToksikДокумент32 страницыStruma Nodulus Non Toksikderahmat dedyОценок пока нет
- Indikasi Dan Kontraindikasi Dekompresi JarumДокумент3 страницыIndikasi Dan Kontraindikasi Dekompresi JarumNurul AtiqahОценок пока нет
- Deresuscitation ARDSДокумент28 страницDeresuscitation ARDSSudaryadiОценок пока нет
- Emergency Management of Severe Burns (EMSB) : Dr. Amrin Amir LubisДокумент17 страницEmergency Management of Severe Burns (EMSB) : Dr. Amrin Amir Lubisamrin amir lubisОценок пока нет
- Otitis MediaДокумент48 страницOtitis MediaRaisah_Ridwan382Оценок пока нет
- 1st Announcement Symposium & Workshop HIPERCCI 2023 FIXДокумент5 страниц1st Announcement Symposium & Workshop HIPERCCI 2023 FIXHakim Danur IqbalОценок пока нет
- Anatomi Dan Fisiologi TidurДокумент25 страницAnatomi Dan Fisiologi TidurMuhammad HidayatОценок пока нет
- Joni DialogДокумент3 страницыJoni DialogJoni TriliwijayaОценок пока нет
- Laporan Kasus TB LaringДокумент39 страницLaporan Kasus TB LaringAditya SahidОценок пока нет
- ASKEP Rheumatoid ArthritisДокумент46 страницASKEP Rheumatoid ArthritisPalupi Setyo HapsariОценок пока нет
- Uts Aena Div Keperawatan Anestesiologi TK II Semester VIДокумент1 страницаUts Aena Div Keperawatan Anestesiologi TK II Semester VIpadila hipzahОценок пока нет
- Perbedaan NNT Pada Trial Effectiveness Dan NNT Trial Adverse EffectДокумент8 страницPerbedaan NNT Pada Trial Effectiveness Dan NNT Trial Adverse EffectUlquiorra SchifferОценок пока нет
- Algoritma Penatalaksanaan Gagal NafasДокумент1 страницаAlgoritma Penatalaksanaan Gagal NafasHairina MazlanОценок пока нет
- 32953182: Physiologically Difficult Airway in The Patient With Severe Hypotension and Metabolic AcidosisДокумент4 страницы32953182: Physiologically Difficult Airway in The Patient With Severe Hypotension and Metabolic AcidosisNico Angelo CopoОценок пока нет
- Myasthenia Gravis ReferatДокумент26 страницMyasthenia Gravis ReferatUlfa TitiswariОценок пока нет
- FotoДокумент1 страницаFotoLion Sangkut Neng EndiОценок пока нет
- Code SampleДокумент1 страницаCode SampleLion Sangkut Neng EndiОценок пока нет
- Kompilasi Laporan Praktikum Farmakognosi I: Akademi Farmasi Samarinda TAHUN 2017/2018Документ1 страницаKompilasi Laporan Praktikum Farmakognosi I: Akademi Farmasi Samarinda TAHUN 2017/2018Lion Sangkut Neng EndiОценок пока нет
- W3j5u-8u66n-D0b9m-54slm - Ec0q6-Qn7uh-5s3jb-Yzmek - Gzljy-X50s3-0s20d-Nfrf9Документ1 страницаW3j5u-8u66n-D0b9m-54slm - Ec0q6-Qn7uh-5s3jb-Yzmek - Gzljy-X50s3-0s20d-Nfrf9Lion Sangkut Neng EndiОценок пока нет
- Implementation of 7s Framenwork On RestuДокумент36 страницImplementation of 7s Framenwork On RestuMuhammad AtaОценок пока нет
- Su Jok, Twist Therapy AND Smile MeditationДокумент7 страницSu Jok, Twist Therapy AND Smile MeditationprateekОценок пока нет
- CV AmosДокумент4 страницыCV Amoscharity busoloОценок пока нет
- Sri Guru Parampara Stotram CompressДокумент14 страницSri Guru Parampara Stotram CompressSatishPavurayalaОценок пока нет
- Binding of IsaacДокумент10 страницBinding of IsaacBraz SouzaОценок пока нет
- Osteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of ChittagongДокумент30 страницOsteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of Chittagongsamiul bashirОценок пока нет
- Symbiosis National Aptitude Test (SNAP) 2004: InstructionsДокумент21 страницаSymbiosis National Aptitude Test (SNAP) 2004: InstructionsHarsh JainОценок пока нет
- Storey Publishing Fall 2017 CatalogДокумент108 страницStorey Publishing Fall 2017 CatalogStorey PublishingОценок пока нет
- Parkinson DiseaseДокумент49 страницParkinson Diseaseiqra100% (1)
- Task Basis JurisprudenceДокумент10 страницTask Basis JurisprudenceKerwin LeonidaОценок пока нет
- Thesis Committee MeetingДокумент7 страницThesis Committee Meetingafknojbcf100% (2)
- Ubi Jus Ibi RemediumДокумент9 страницUbi Jus Ibi RemediumUtkarsh JaniОценок пока нет
- Soal Midtest + Kunci JawabanДокумент28 страницSoal Midtest + Kunci JawabanYuyun RasulongОценок пока нет
- Individual Psychology (Adler)Документ7 страницIndividual Psychology (Adler)manilyn dacoОценок пока нет
- Nguyễn Thị Ngọc Huyền - 19125516 - Homework 3Документ7 страницNguyễn Thị Ngọc Huyền - 19125516 - Homework 3Nguyễn HuyềnОценок пока нет
- 7 - LESSON PLAN CULTURAL HERITAGE AND CULTURAL DIVERSITY - Lesson PlanДокумент4 страницы7 - LESSON PLAN CULTURAL HERITAGE AND CULTURAL DIVERSITY - Lesson PlanRute SobralОценок пока нет
- Rizal ExaminationДокумент3 страницыRizal ExaminationBea ChristineОценок пока нет
- Spyderco Product Guide - 2016Документ154 страницыSpyderco Product Guide - 2016marceudemeloОценок пока нет
- Navamsa Karma and GodДокумент9 страницNavamsa Karma and GodVisti Larsen50% (2)
- CURRICULUM VITAE Kham Khan Suan Hausing, PHDДокумент8 страницCURRICULUM VITAE Kham Khan Suan Hausing, PHDCinpu ZomiОценок пока нет
- Paradigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportДокумент5 страницParadigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportPsychology and Education: A Multidisciplinary JournalОценок пока нет
- ThesisДокумент58 страницThesisTirtha Roy BiswasОценок пока нет
- Tamil Ilakkanam Books For TNPSCДокумент113 страницTamil Ilakkanam Books For TNPSCkk_kamalakkannan100% (1)
- 9.2 Volumetric Analysis PDFДокумент24 страницы9.2 Volumetric Analysis PDFJoaquinОценок пока нет
- Strategi Pencegahan Kecelakaan Di PT VALE Indonesia Presentation To FPP Workshop - APKPI - 12102019Документ35 страницStrategi Pencegahan Kecelakaan Di PT VALE Indonesia Presentation To FPP Workshop - APKPI - 12102019Eko Maulia MahardikaОценок пока нет
- Assignment Submission Form: Pgid Name of The MemberДокумент9 страницAssignment Submission Form: Pgid Name of The MemberNamit GaurОценок пока нет
- Ross, D. (2013) - Field Guide To Jumping Spiders of Southeast Idaho.Документ4 страницыRoss, D. (2013) - Field Guide To Jumping Spiders of Southeast Idaho.Dave RossОценок пока нет
- Radiopharmaceutical Production: History of Cyclotrons The Early Years at BerkeleyДокумент31 страницаRadiopharmaceutical Production: History of Cyclotrons The Early Years at BerkeleyNguyễnKhươngDuyОценок пока нет
- 1sebastian Vs CalisДокумент6 страниц1sebastian Vs CalisRai-chan Junior ÜОценок пока нет
- Muller-Lyer IllusionДокумент3 страницыMuller-Lyer Illusionsara VermaОценок пока нет