Вам также может понравиться
- Cranial Nerve AssessmentДокумент42 страницыCranial Nerve AssessmentValeryn Quiman100% (8)
- Cranial Nerves ExamДокумент58 страницCranial Nerves ExamTom JenyonОценок пока нет
- NeurologyДокумент5 страницNeurologyES AbedОценок пока нет
- Wall Neuro 2010Документ34 страницыWall Neuro 2010Kath Jacinto100% (1)
- Clinical OSCE Notes PDFДокумент49 страницClinical OSCE Notes PDFArwa QishtaОценок пока нет
- Dysphagia Case History: Chart ReviewДокумент24 страницыDysphagia Case History: Chart ReviewTiffani Wallace75% (4)
- Visual PathwayДокумент24 страницыVisual PathwayAkshara Eye FoundationОценок пока нет
- Cranial Nerve Exam Part1Документ9 страницCranial Nerve Exam Part1Jennifer Pisco LiracОценок пока нет
- ASIA Impairment ScaleДокумент10 страницASIA Impairment Scaleazimahzainal211Оценок пока нет
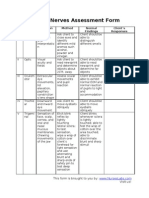
- Cranial Nerves Assessment FormДокумент3 страницыCranial Nerves Assessment Formmhel03_chickmagnetОценок пока нет
- Head Injury - HandoutДокумент10 страницHead Injury - HandoutMohd Hisyamuddin SaharudinОценок пока нет
- Trigeminal NeuralgiaДокумент48 страницTrigeminal NeuralgiaSonia Bhansali100% (4)
- Superficial and Deep ReflexesДокумент28 страницSuperficial and Deep ReflexesShilpa SОценок пока нет
- Tract Continues Down Spinal Cord: Input Location Notes Lesion MedullaДокумент10 страницTract Continues Down Spinal Cord: Input Location Notes Lesion MedullaherethemindОценок пока нет
- Higher Center - Dr. BarbonДокумент5 страницHigher Center - Dr. BarbonMelissa SalayogОценок пока нет
- Neuromuscular: Cranial NervesДокумент30 страницNeuromuscular: Cranial NerveswanderlastОценок пока нет
- Neurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemДокумент29 страницNeurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemDarla Mitu100% (2)
- Anatomy & Physiology NSДокумент73 страницыAnatomy & Physiology NSIsha Bhusal67% (3)
- Cranial Nerves: DR Dyan Roshinta Laksmi Dewi, SP.S SMF Saraf Rsud DR Soedarso PontianakДокумент19 страницCranial Nerves: DR Dyan Roshinta Laksmi Dewi, SP.S SMF Saraf Rsud DR Soedarso PontianakVidia AsriyantiОценок пока нет
- Nervous System PathologyДокумент57 страницNervous System Pathologypatriciasuscking100% (1)
- Brain Areas - Location and FunctionДокумент12 страницBrain Areas - Location and FunctionMattGilmoreОценок пока нет
- Medical Surgical Nursing Review NotesДокумент75 страницMedical Surgical Nursing Review NotesMary Ann Comia RañolaОценок пока нет
- Approach To Unconsious PTДокумент62 страницыApproach To Unconsious PTHussain AzharОценок пока нет
- Quick Review of Cranial Nerves: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMДокумент32 страницыQuick Review of Cranial Nerves: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMShintaОценок пока нет
- Bell's Palsy EbnДокумент48 страницBell's Palsy EbnClara Maey GarciaОценок пока нет
- Clinical Massage Therapy Understanding, Assessing and Treating Over 70 Conditions (PDFDrive)Документ1 142 страницыClinical Massage Therapy Understanding, Assessing and Treating Over 70 Conditions (PDFDrive)alexandruomeОценок пока нет
- Dermatomes & Myotomes PDFДокумент4 страницыDermatomes & Myotomes PDFsridhar_physio0% (1)
- Somatosensory SystemДокумент34 страницыSomatosensory SystemMicko Martha ThamrinОценок пока нет
- Erman Fandialan M.D. Department of Clinical Neurosciences UermmmcДокумент48 страницErman Fandialan M.D. Department of Clinical Neurosciences Uermmmclovelots1234100% (1)
- Spinal InjuriesДокумент22 страницыSpinal InjuriesPak Budi warsonoОценок пока нет
- CVS PDFДокумент102 страницыCVS PDFmalik003Оценок пока нет
- 1000 Prometric MCQ Solved 2Документ351 страница1000 Prometric MCQ Solved 2chronos653490% (106)
- Head To Toe AssessmentДокумент22 страницыHead To Toe AssessmentNessa Layos MorilloОценок пока нет
- Multiple SclerosisДокумент43 страницыMultiple SclerosisProdan SimonaОценок пока нет
- Latest Dr. Saleh Facial Nerve Applied 16.5.23Документ85 страницLatest Dr. Saleh Facial Nerve Applied 16.5.23Saleh Mohammad ShoaibОценок пока нет
- Neurology ConferenceДокумент59 страницNeurology ConferencePGHC100% (4)
- Dha Exam..Muhammad IbrahimДокумент11 страницDha Exam..Muhammad Ibrahimmalik003100% (4)
- Neurologic Disorder: By: Sandot, Alfrien BДокумент118 страницNeurologic Disorder: By: Sandot, Alfrien BNeirfla WassabiОценок пока нет
- Assessment of Neurological SystemДокумент26 страницAssessment of Neurological SystemBatiao Camille Claire100% (1)
- Endodontics Old Textbook Qs SearchableДокумент45 страницEndodontics Old Textbook Qs Searchablejentothesky90% (10)
- Cranial Nerve Exam in DetailДокумент36 страницCranial Nerve Exam in DetailANIE100% (1)
- The Motor System ExaminationДокумент42 страницыThe Motor System ExaminationHelend ChildDj100% (1)
- Neuro AssessmentДокумент3 страницыNeuro AssessmentTori RolandОценок пока нет
- Rinne WeberДокумент3 страницыRinne WeberbenlarsenaОценок пока нет
- Cranialnerveassessmentfinal 140501113414 Phpapp01 PDFДокумент42 страницыCranialnerveassessmentfinal 140501113414 Phpapp01 PDFAlma Baterina100% (1)
- Cogan Syndrome Surger 4, AnkitДокумент18 страницCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyОценок пока нет
- Chronic SinusitisДокумент19 страницChronic SinusitisMunawwar AwaОценок пока нет
- Neurology II Second Long Exam 2014AДокумент14 страницNeurology II Second Long Exam 2014Acbac1990Оценок пока нет
- Anatomy - Scalp PDFДокумент3 страницыAnatomy - Scalp PDFAngel Kim100% (1)
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids) : Analgesic, Anti-Pyretic and Anti-Inflammatory AgentsДокумент45 страницNon-Steroidal Anti-Inflammatory Drugs (Nsaids) : Analgesic, Anti-Pyretic and Anti-Inflammatory AgentsArvi KhanОценок пока нет
- Medrano Neuro Notes 2.0Документ22 страницыMedrano Neuro Notes 2.0roldan pantojaОценок пока нет
- Development of GITДокумент88 страницDevelopment of GITBindiya MangarОценок пока нет
- Nervous System Examination SynopsisДокумент26 страницNervous System Examination Synopsisaarti chandeОценок пока нет
- PBL NCM 112 2nd ROTATIONДокумент3 страницыPBL NCM 112 2nd ROTATIONLeanne Princess Gamboa100% (1)
- 19 Neuromuscular DisordersДокумент39 страниц19 Neuromuscular DisordersSara 'Yaa SaraaОценок пока нет
- Facial Nerve Palsy: Dr. Saud AlromaihДокумент74 страницыFacial Nerve Palsy: Dr. Saud AlromaihChandra ManapaОценок пока нет
- Case Writeup Albert Labores 9.24.2010 StrokeДокумент6 страницCase Writeup Albert Labores 9.24.2010 StrokeAJ RegaladoОценок пока нет
- Supra Nuclear Eye Movement SystemДокумент57 страницSupra Nuclear Eye Movement SystemPrashob MohanОценок пока нет
- General Pathology For Medical StudentsДокумент225 страницGeneral Pathology For Medical Studentsscousevet100% (1)
- ANA 6.01 General Somatic Afferents Dr. EsguerraДокумент22 страницыANA 6.01 General Somatic Afferents Dr. EsguerraNinna Ricci San JuanОценок пока нет
- JIMENEZ, Joseph M. Neurology Preceptorial 2019A March 2, 2018Документ6 страницJIMENEZ, Joseph M. Neurology Preceptorial 2019A March 2, 2018John PaguidianОценок пока нет
- Use The Following Criteria in Evaluating The Skill PerformanceДокумент4 страницыUse The Following Criteria in Evaluating The Skill Performancekookie100% (1)
- Urinary System Disorders Practice Quiz #1 (50 Questions)Документ26 страницUrinary System Disorders Practice Quiz #1 (50 Questions)Emy TandinganОценок пока нет
- Cranial Nerves: Hemachandran G Bot 2 Year RA1821002010077Документ17 страницCranial Nerves: Hemachandran G Bot 2 Year RA1821002010077HEMA CHANDRAN100% (1)
- Cranial Nerve 6, 7 and 8 (Short Presentation)Документ33 страницыCranial Nerve 6, 7 and 8 (Short Presentation)3uvpОценок пока нет
- 12.basal Nuclei PDFДокумент3 страницы12.basal Nuclei PDFadiОценок пока нет
- CherubismДокумент12 страницCherubismSureeratPatima100% (1)
- Practicals Histology Prelims AДокумент36 страницPracticals Histology Prelims AShaylla BretañaОценок пока нет
- Cerebellar Function Tests: Experiment 29: Md-1C Group 5Документ42 страницыCerebellar Function Tests: Experiment 29: Md-1C Group 5Verlette Roselle Aguisanda LizardoОценок пока нет
- Neurological ExaminationДокумент32 страницыNeurological ExaminationJuling PeralesОценок пока нет
- Extrapyramidal SystemДокумент23 страницыExtrapyramidal SystemALTAN26Оценок пока нет
- Neurological ExaminationДокумент71 страницаNeurological ExaminationSiti Nursuhada binti Mohd AminОценок пока нет
- Recent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A ReviewДокумент18 страницRecent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A Reviewmalik003Оценок пока нет
- History in Ob/Gy: Ahmed AbdulwahabДокумент9 страницHistory in Ob/Gy: Ahmed Abdulwahabmalik003Оценок пока нет
- VascularDisordersLiver2009 PDFДокумент36 страницVascularDisordersLiver2009 PDFmalik003Оценок пока нет
- SummariesДокумент140 страницSummariesmalik003Оценок пока нет
- Career Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017Документ2 страницыCareer Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017malik003Оценок пока нет
- Recommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29Документ8 страницRecommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29malik003Оценок пока нет
- Recommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29Документ12 страницRecommendations For Testing, Managing, and Treating Hepatitis C - HCV TESTING and LINKAGE To CARE - 2015-06-29malik003Оценок пока нет
- Visa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSДокумент1 страницаVisa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSmalik003Оценок пока нет
- Bleeding Disorder ApproachДокумент9 страницBleeding Disorder Approachmalik003Оценок пока нет
- GR 080013Документ3 страницыGR 080013malik003Оценок пока нет
- April 24: Zein Mahgoub PACES Simplified Zein MahgoubДокумент4 страницыApril 24: Zein Mahgoub PACES Simplified Zein Mahgoubmalik003Оценок пока нет
- Unilateral Enlarged Kidney PDFДокумент2 страницыUnilateral Enlarged Kidney PDFmalik003Оценок пока нет
- Prevention of Venous Thromboembolism in Nonsurgical PatientsДокумент23 страницыPrevention of Venous Thromboembolism in Nonsurgical Patientsmalik003Оценок пока нет
- Urgent Required Female Staff NursesДокумент1 страницаUrgent Required Female Staff Nursesmalik003Оценок пока нет
- 6868841Документ35 страниц6868841malik003Оценок пока нет
- Associate Med PDFДокумент2 страницыAssociate Med PDFmalik003Оценок пока нет
- 5446.full 2Документ12 страниц5446.full 2malik003Оценок пока нет
- New Doc 44 - 1Документ1 страницаNew Doc 44 - 1malik003Оценок пока нет
- Assoc Prof MedДокумент1 страницаAssoc Prof Medmalik003Оценок пока нет
- Associate MedДокумент2 страницыAssociate Medmalik003Оценок пока нет
- Branches of Trigeminal Nerve + ForamenДокумент2 страницыBranches of Trigeminal Nerve + Foramen1bsbfanОценок пока нет
- Sensation Kinds and Types of Sensory Disturbance Syndromes of LesionДокумент67 страницSensation Kinds and Types of Sensory Disturbance Syndromes of LesionAhmed Adel SaadОценок пока нет
- Cranial Nerve V - Trigeminal Nerve - FRCEM SuccessДокумент1 страницаCranial Nerve V - Trigeminal Nerve - FRCEM SuccessJohn CoxОценок пока нет
- Group 6 - Nervous Sytem PresentationДокумент157 страницGroup 6 - Nervous Sytem PresentationNgirlОценок пока нет
- Final Exam in Topographical AnatomyДокумент50 страницFinal Exam in Topographical Anatomytastyk100% (2)
- A59. Brain Stem LESIONSДокумент8 страницA59. Brain Stem LESIONSMariana AmbossОценок пока нет
- MeningiomaДокумент7 страницMeningiomadrhendyjuniorОценок пока нет
- Cranial Nerve ExamДокумент20 страницCranial Nerve ExamSIR ONEОценок пока нет
- Review The Relationship Between The Stomatognathic System and Body PostureДокумент6 страницReview The Relationship Between The Stomatognathic System and Body PosturemarcelonorisОценок пока нет
- Central Mindanao University: Scale Description Interpretation Assistance NeededДокумент2 страницыCentral Mindanao University: Scale Description Interpretation Assistance NeededBrandon Sydnee GonzalesОценок пока нет
- Medicowesome Deviation of The Tongue, Jaw, Uvula 2Документ1 страницаMedicowesome Deviation of The Tongue, Jaw, Uvula 2KC Dela RosaОценок пока нет
- WORKSHOP No 2Документ25 страницWORKSHOP No 2Jose QuintoОценок пока нет
- GV26 Acupuncture Emergency PointДокумент4 страницыGV26 Acupuncture Emergency PointJosé Mário100% (1)
- LWW BATES 17 CranialMotorSystem Transcript FINALДокумент8 страницLWW BATES 17 CranialMotorSystem Transcript FINALRachel Lalaine Marie SialanaОценок пока нет
- Clinical SkillsДокумент11 страницClinical SkillsAhmad SobihОценок пока нет
- Interventional Pain ManagementДокумент66 страницInterventional Pain ManagementFajar ShodiqОценок пока нет
- Cranial NervesДокумент40 страницCranial NervesStephanie ArceoОценок пока нет
- Managing Lockjaw Disorders in Dogs: TrismusДокумент14 страницManaging Lockjaw Disorders in Dogs: TrismusmiloОценок пока нет
- Trigeminal and Facial NerveДокумент121 страницаTrigeminal and Facial NerveFadilaОценок пока нет
- 1general SensationДокумент141 страница1general SensationAzimuddeen AzeliОценок пока нет
- 3-1. Diagnosis Topis Neurologi (Dr. Iqbal Basri, SP.S)Документ48 страниц3-1. Diagnosis Topis Neurologi (Dr. Iqbal Basri, SP.S)FitrianiОценок пока нет