Вам также может понравиться
- Lecture Notes Finals RT 208Документ5 страницLecture Notes Finals RT 208Giralph NikkoОценок пока нет
- Physics of RadiationДокумент8 страницPhysics of Radiationalialahmedy24Оценок пока нет
- Basics of Radiation Therapy: Ryan K. Funk,, Abigail L. Stockham,, Nadia N. Issa LaackДокумент22 страницыBasics of Radiation Therapy: Ryan K. Funk,, Abigail L. Stockham,, Nadia N. Issa LaackAlejo RLОценок пока нет
- Lecture 2Документ53 страницыLecture 2stopОценок пока нет
- Radiation Protection & Quality Assurance in CT 2018Документ51 страницаRadiation Protection & Quality Assurance in CT 2018abafzОценок пока нет
- Chapter - 2-Biological Effects of Ionizing RadiationДокумент25 страницChapter - 2-Biological Effects of Ionizing RadiationHayat MuljanaОценок пока нет
- Application of Radiobiology in RTДокумент61 страницаApplication of Radiobiology in RTnilesh kumarОценок пока нет
- Detecting and Measuring Radiation Lect 4Документ22 страницыDetecting and Measuring Radiation Lect 4Tonyo LinaОценок пока нет
- 01 Radiation UnitsДокумент41 страница01 Radiation UnitsFakhrul SyukriОценок пока нет
- RADIOBIOLOGY Speaker Sharib Ahmed On 19-11-2013Документ32 страницыRADIOBIOLOGY Speaker Sharib Ahmed On 19-11-2013Waqar Ahmed0% (1)
- Introduction To Nuclear Medicine: Sania Rahim PGY 4 BCM C/o 2008Документ28 страницIntroduction To Nuclear Medicine: Sania Rahim PGY 4 BCM C/o 2008asfadsi23Оценок пока нет
- Non-Ionizing Radiation: DR Rudy Foddis Occupational Medicine Medicine and Surgery Faculty University of PisaДокумент29 страницNon-Ionizing Radiation: DR Rudy Foddis Occupational Medicine Medicine and Surgery Faculty University of PisamohammedОценок пока нет
- Curriculum Physics RadiologyДокумент156 страницCurriculum Physics Radiologydrzalie70Оценок пока нет
- Physical Principles of UtzДокумент44 страницыPhysical Principles of UtzRalph RichardОценок пока нет
- Chapter (2) Part (1) 15-11-2021Документ38 страницChapter (2) Part (1) 15-11-2021Ahmed HamdyОценок пока нет
- 4 Background RadiationДокумент1 страница4 Background Radiationsomu1100% (1)
- Occupational Radiation Safety: Directed Readings in The ClassroomДокумент54 страницыOccupational Radiation Safety: Directed Readings in The ClassroomErick Calcaligong100% (2)
- Radiation - Quantities and Units of Ionizing RadiationДокумент7 страницRadiation - Quantities and Units of Ionizing RadiationjamessonianОценок пока нет
- Ultra High Field Magnetic Resonance ImagingДокумент487 страницUltra High Field Magnetic Resonance ImagingEduardoAndresChacamaVernalОценок пока нет
- Protection From RadiationДокумент8 страницProtection From Radiationapi-270822363Оценок пока нет
- European Guidelines On Quality Criteria For Computed Tomography PDFДокумент2 страницыEuropean Guidelines On Quality Criteria For Computed Tomography PDFBennettОценок пока нет
- Understanding BrachytherapyДокумент28 страницUnderstanding Brachytherapyqwertu132Оценок пока нет
- 2 Fundamental Principles of RadiobiologyДокумент28 страниц2 Fundamental Principles of RadiobiologyAngelo RamosОценок пока нет
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyДокумент96 страниц2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniОценок пока нет
- Radiation Physics and DosimetryДокумент21 страницаRadiation Physics and DosimetryAlexis Nathán RuedaОценок пока нет
- Radiation Biology: Presented By: Aarya.H.NairДокумент83 страницыRadiation Biology: Presented By: Aarya.H.NairAARYAОценок пока нет
- Resident Physics Lectures: Radiography GeometryДокумент36 страницResident Physics Lectures: Radiography GeometryLajja Parikh PatelОценок пока нет
- Body Basic - PpsДокумент136 страницBody Basic - PpsRadiologi Mika bintaroОценок пока нет
- Radiopharmaceuticals (Journal) PDFДокумент6 страницRadiopharmaceuticals (Journal) PDFFrederickОценок пока нет
- Personnel Monitoring DevicesДокумент63 страницыPersonnel Monitoring DevicesPramod Tike100% (1)
- Radiopharmaceuticsdrmallhi 160425162404Документ39 страницRadiopharmaceuticsdrmallhi 160425162404Khalid HussainОценок пока нет
- Interaction of Radiation With MatterДокумент16 страницInteraction of Radiation With MatterRachit KanchanОценок пока нет
- Module - I: JurisprudenceДокумент10 страницModule - I: JurisprudenceReygil CapunoОценок пока нет
- Powerpoint Lecture in Mri (2) (Autosaved) - 1Документ167 страницPowerpoint Lecture in Mri (2) (Autosaved) - 1Ralph AbetoОценок пока нет
- Solutions: Radiation Medicine QaДокумент128 страницSolutions: Radiation Medicine QaHashir SaeedОценок пока нет
- Biological Effects of Radiation IAEAДокумент87 страницBiological Effects of Radiation IAEAkhushi786100% (1)
- MRI SafetyДокумент42 страницыMRI SafetyadamayhalОценок пока нет
- Radiation Therapy Physics by George T. Y. Chen PHD, Charles A. Pelizzari PHD (Auth.), Alfred R. Smith PHD (Eds.)Документ468 страницRadiation Therapy Physics by George T. Y. Chen PHD, Charles A. Pelizzari PHD (Auth.), Alfred R. Smith PHD (Eds.)Augusto KiyoshiОценок пока нет
- Health PhysicsДокумент33 страницыHealth Physicsg1381821Оценок пока нет
- Review of Electron Beam Therapy PhysicsДокумент36 страницReview of Electron Beam Therapy PhysicsMaría José Sánchez LovellОценок пока нет
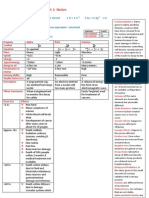
- 2922radioactivity Summary Cheat Sheet..Aidan MatthewsДокумент3 страницы2922radioactivity Summary Cheat Sheet..Aidan MatthewsSyed Mairaj Ul HaqОценок пока нет
- Radiation ProtectionДокумент37 страницRadiation Protectionlogofwood6858Оценок пока нет
- Mobile Tower and Mobile Phone Radiation Hazards - Prof Girish KumarДокумент52 страницыMobile Tower and Mobile Phone Radiation Hazards - Prof Girish KumarNeha KumarОценок пока нет
- Raphex Answers 2010Документ15 страницRaphex Answers 2010Ant MenОценок пока нет
- Radiation Protection 2Документ23 страницыRadiation Protection 2samndarkhanОценок пока нет
- Flouroscopy: DR Rubeena Ali Senior Registrar Radiology Department Rlmc/AmthДокумент96 страницFlouroscopy: DR Rubeena Ali Senior Registrar Radiology Department Rlmc/AmthMuhammad WasifОценок пока нет
- Ch. 37 Biomedical PhyДокумент23 страницыCh. 37 Biomedical PhyMahmoud Abu MayalehОценок пока нет
- 01 - Radiation Protection 1 - WM 2013Документ42 страницы01 - Radiation Protection 1 - WM 2013Amr MuhammedОценок пока нет
- Chapter 01 Basics Radiation PhysicsДокумент195 страницChapter 01 Basics Radiation PhysicsJose Ivan MejiaОценок пока нет
- Chapter 02 Dosimetric PrinciplesДокумент131 страницаChapter 02 Dosimetric PrinciplesLida Velasquez SierraОценок пока нет
- Radiation DosimetryДокумент18 страницRadiation DosimetrySmita SharmaОценок пока нет
- Ultrasounds of The Thyroid and Parathyroid GlandsДокумент12 страницUltrasounds of The Thyroid and Parathyroid GlandsDianita RiofrioОценок пока нет
- Radiation Biology LectureДокумент39 страницRadiation Biology LectureBipin UpadhyayОценок пока нет
- Radiation ProtectionДокумент50 страницRadiation ProtectionDragan GigiОценок пока нет
- Brachytherapy Techniques: Surface MouldДокумент9 страницBrachytherapy Techniques: Surface MouldpawanОценок пока нет
- Basic radiobiology: fractionation, 5 Rs, α/β ratio, QUANTEC: ESO Masterclass in Oncology Basics for BeginnersДокумент32 страницыBasic radiobiology: fractionation, 5 Rs, α/β ratio, QUANTEC: ESO Masterclass in Oncology Basics for BeginnersAji PatriajatiОценок пока нет
- RadiobiologyДокумент70 страницRadiobiologypia toledoОценок пока нет
- Introduction To MRIДокумент16 страницIntroduction To MRIjuhiОценок пока нет
- KN Govinda - Radiation Safety in Radiation OncologyДокумент455 страницKN Govinda - Radiation Safety in Radiation OncologyMaranda RoleaОценок пока нет
- Computer Based Industrial ControlДокумент625 страницComputer Based Industrial ControlLiviu100% (1)
- Ansi C57.92 TrafoДокумент28 страницAnsi C57.92 Trafoliheber100% (2)
- Sanet - ST Control20Systems PDFДокумент364 страницыSanet - ST Control20Systems PDFLiviuОценок пока нет
- Sanet - ST - 1871962552 - Mike JamesДокумент314 страницSanet - ST - 1871962552 - Mike JamesLiviuОценок пока нет
- Simatic DiplomaДокумент1 страницаSimatic DiplomaLiviuОценок пока нет
- CEDO - Prima de Vacanta PDFДокумент1 страницаCEDO - Prima de Vacanta PDFLiviuОценок пока нет
- Sanet - ST - 1871962544 - Mike JamesДокумент320 страницSanet - ST - 1871962544 - Mike JamesLiviuОценок пока нет
- Transformer Winding Hot Spot Temperature DeterminationДокумент35 страницTransformer Winding Hot Spot Temperature Determinationlbk50Оценок пока нет
- Sanet - ST 1447110552 PHPДокумент559 страницSanet - ST 1447110552 PHPLiviuОценок пока нет
- Advanced Visual Basic 6 Power Techniques For Everyday Programs.9780201707120.24922Документ515 страницAdvanced Visual Basic 6 Power Techniques For Everyday Programs.9780201707120.24922rajeshsasi100% (2)
- Speech-Enabling Visual Basic 6 Applications With Microsoft SAPI 5.1Документ10 страницSpeech-Enabling Visual Basic 6 Applications With Microsoft SAPI 5.1LiviuОценок пока нет
- Delphi Database Programming With ADOДокумент231 страницаDelphi Database Programming With ADOZack GithinjiОценок пока нет
- Beautiful PaintingsДокумент3 страницыBeautiful PaintingsLiviuОценок пока нет
- Make Your Own GUI in ExcelДокумент17 страницMake Your Own GUI in ExcelLiviu100% (1)
- SAnet Me Blender3DABeginners15StepExerciseДокумент83 страницыSAnet Me Blender3DABeginners15StepExerciseLiviuОценок пока нет
- Vb6 PreviewДокумент26 страницVb6 PreviewonkarsdatarОценок пока нет
- Net TruePDF JuneДокумент118 страницNet TruePDF Junedress tgh100% (1)
- ADRESEДокумент3 страницыADRESELiviuОценок пока нет
- PHP The Ultimate Step by Step Guide For BeginnersДокумент182 страницыPHP The Ultimate Step by Step Guide For BeginnersAnonymous 6WUzAScL2100% (1)
- Microsoft Visual Basic 6.0: Applied ScienceДокумент54 страницыMicrosoft Visual Basic 6.0: Applied ScienceAsma HassanОценок пока нет
- Mastering Mathematics For Electronic EngineeringДокумент397 страницMastering Mathematics For Electronic EngineeringLiviu100% (2)
- Visual Basic Brief IntroДокумент48 страницVisual Basic Brief IntroheloverОценок пока нет
- Excel Formulas PDFДокумент163 страницыExcel Formulas PDFLiviuОценок пока нет
- Introduction To Nuclear Weapon Physics and DesignДокумент14 страницIntroduction To Nuclear Weapon Physics and DesignLiviu100% (1)
- How To Create An AppДокумент47 страницHow To Create An AppLiviuОценок пока нет
- How To Install and Use Custom 3rd Party Themes in WindowsДокумент7 страницHow To Install and Use Custom 3rd Party Themes in WindowsLiviuОценок пока нет
- Make Your Own GUI in ExcelДокумент17 страницMake Your Own GUI in ExcelLiviu100% (1)
- 1SDC010001D0201 PDFДокумент117 страниц1SDC010001D0201 PDFDidik RiswantoОценок пока нет
- PM1610 - Leaflet (2023.04)Документ2 страницыPM1610 - Leaflet (2023.04)Роман РакусовОценок пока нет
- Radio PharmaceuticalsДокумент31 страницаRadio PharmaceuticalsGail AidОценок пока нет
- Iaea Tecdoc 1622Документ249 страницIaea Tecdoc 1622mrudelliОценок пока нет
- Nuclear Tech English - PDFДокумент20 страницNuclear Tech English - PDFShivang BhardwajОценок пока нет
- Assignment No-1 Simulation and Modelling of Solar PV Pannel: TheoryДокумент7 страницAssignment No-1 Simulation and Modelling of Solar PV Pannel: Theorypooja chirdeОценок пока нет
- Solis Power Solution - Solar Project Installation JaipurДокумент2 страницыSolis Power Solution - Solar Project Installation JaipurSolis PowerОценок пока нет
- Radioisotopes in IndustryДокумент13 страницRadioisotopes in IndustryChris Tine ChiaОценок пока нет
- Radiation Heat TranferДокумент30 страницRadiation Heat TranferAkash MishraОценок пока нет
- Tutorial 1Документ3 страницыTutorial 1muhammad haziqОценок пока нет
- EBM Presentation Natasha - ANAS - NewДокумент15 страницEBM Presentation Natasha - ANAS - NewSyed Umair HashmiОценок пока нет
- Hi-Scan OverviewДокумент46 страницHi-Scan OverviewJose SoaresОценок пока нет
- Electron Interaction With MatterДокумент14 страницElectron Interaction With MatterVinche CanalijaОценок пока нет
- Radiation Physics and Dosimetry: Institute of Radiation Safety, Sudan Atomic Energy CommissionДокумент51 страницаRadiation Physics and Dosimetry: Institute of Radiation Safety, Sudan Atomic Energy CommissionOmar A. MohammadОценок пока нет
- Mysterious Attack in The Southern BeachДокумент1 страницаMysterious Attack in The Southern BeachI'm SyasyeeОценок пока нет
- Radiation ProtectionДокумент56 страницRadiation ProtectionYessamae JinangОценок пока нет
- 8.1 Discovery of RadioactivityДокумент6 страниц8.1 Discovery of RadioactivitysyaОценок пока нет
- Edexcel Nuclear Energy QPДокумент19 страницEdexcel Nuclear Energy QPLithmi KarunanayakeОценок пока нет
- Radio-Analytical TechniquesДокумент30 страницRadio-Analytical TechniquesMohammad Zamir TaqwaОценок пока нет
- Final 00086Документ7 страницFinal 00086kurniawan waskitoОценок пока нет
- Solar EnergyДокумент13 страницSolar EnergyArun GaneshОценок пока нет
- NCRP Report 133 IndexДокумент4 страницыNCRP Report 133 IndexEng.AymanОценок пока нет
- Science 6 Q3 W4 LAS 3Документ2 страницыScience 6 Q3 W4 LAS 3Ellen Jenneth PudaОценок пока нет
- An Introduction To Radiation ProtectionДокумент259 страницAn Introduction To Radiation ProtectionNabaaAlazawy89% (9)
- 1698414914671Документ71 страница1698414914671michele.raimo24Оценок пока нет
- Solar Energy PDFДокумент22 страницыSolar Energy PDFKaushiki KambojОценок пока нет
- Gamma Ray Bursters Spectrum of RadiationДокумент139 страницGamma Ray Bursters Spectrum of RadiationVincent J. CataldiОценок пока нет
- GWCC1Документ2 страницыGWCC1Aastha SinghОценок пока нет
- Radiology and Radiation SafetyДокумент4 страницыRadiology and Radiation Safetycoordinator.dargaiОценок пока нет
- Nuclear Decay QuestionДокумент2 страницыNuclear Decay QuestionDhanBahadurОценок пока нет
- Basic Requirements On Area Dosemeters: Design and Type Test RequirementsДокумент27 страницBasic Requirements On Area Dosemeters: Design and Type Test RequirementsDwi AngestiОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Оценок пока нет
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassОт EverandTroubled: A Memoir of Foster Care, Family, and Social ClassРейтинг: 4.5 из 5 звезд4.5/5 (27)