Вам также может понравиться
- Drug LisinoprilДокумент1 страницаDrug LisinoprilSrkocherОценок пока нет
- LabetalolДокумент3 страницыLabetalolTri Purma Sari50% (2)
- Glipizide Glucotrol XL Drug CardДокумент1 страницаGlipizide Glucotrol XL Drug CardSheri490Оценок пока нет
- Methocarbamol (Robaxin)Документ1 страницаMethocarbamol (Robaxin)EОценок пока нет
- Terazosin Hytrin Drug CardДокумент1 страницаTerazosin Hytrin Drug CardSheri490Оценок пока нет
- Escitalopram OxalateДокумент3 страницыEscitalopram Oxalateapi-3797941Оценок пока нет
- OfloxacinДокумент2 страницыOfloxacinCarla Arciaga100% (1)
- Drug Card BenadrylДокумент1 страницаDrug Card BenadrylAdrianne Bazo100% (1)
- Atropine Drug ProfileДокумент2 страницыAtropine Drug ProfileShahpmdОценок пока нет
- Drug Study - AmlodipineДокумент1 страницаDrug Study - AmlodipineDanielle Marie SamblacenoОценок пока нет
- Test Bank For Basic Pharmacology For Nursing 17th EditionДокумент10 страницTest Bank For Basic Pharmacology For Nursing 17th EditionUsman HaiderОценок пока нет
- MethylprednisoloneДокумент4 страницыMethylprednisoloneadryananestesiОценок пока нет
- Lyrica (Pregabalin)Документ2 страницыLyrica (Pregabalin)Laromac RolandОценок пока нет
- Filgastrim (GCSF)Документ3 страницыFilgastrim (GCSF)Kyla Barrera TabungarОценок пока нет
- Act Rapid 2Документ2 страницыAct Rapid 2Leah Torcelino-InfanteОценок пока нет
- NeostigmineДокумент4 страницыNeostigmineDonna Lyn B. DizonОценок пока нет
- College of Nursing: Cebu Normal UniversityДокумент5 страницCollege of Nursing: Cebu Normal UniversityChelsea WuОценок пока нет
- Chlorpheniramine Maleate: (klor-fen-AIR-uh-meen MAL-ee-ate)Документ4 страницыChlorpheniramine Maleate: (klor-fen-AIR-uh-meen MAL-ee-ate)Nurginayah RusliОценок пока нет
- EsmololДокумент2 страницыEsmololtherock316_995149Оценок пока нет
- THEOPHYLLINE - Drug StudyДокумент2 страницыTHEOPHYLLINE - Drug Studyeric macabiogОценок пока нет
- LidocaineДокумент2 страницыLidocaineAhprelle Quiring Rodiel100% (1)
- Pseudoephedrine HydrochlorideДокумент6 страницPseudoephedrine HydrochlorideAbdelrhman AboodaОценок пока нет
- Tinidazole Drug StudyДокумент2 страницыTinidazole Drug StudyEmagra AzilОценок пока нет
- AcetazolamideДокумент2 страницыAcetazolamideAlexandra Antondy0% (1)
- DapagliflozinДокумент1 страницаDapagliflozinAusaf AhmadОценок пока нет
- Methyldopa, Losartan K, Ascorbic AcidДокумент4 страницыMethyldopa, Losartan K, Ascorbic AcidRico Mae ValenciaОценок пока нет
- Drug Study - BaclofenДокумент5 страницDrug Study - BaclofenRocco WalksОценок пока нет
- Drug Study...Документ5 страницDrug Study...Ezra Dizon ManzanoОценок пока нет
- Doxazosin MesylateДокумент2 страницыDoxazosin Mesylateapi-3797941Оценок пока нет
- EsmololДокумент3 страницыEsmololTri Purma SariОценок пока нет
- Ofloxacin Drug StudyДокумент4 страницыOfloxacin Drug StudyMikko Anthony Pingol Alarcon100% (1)
- Drug StudyДокумент6 страницDrug StudyArdrina SappariОценок пока нет
- Phenergan (Promethazine)Документ1 страницаPhenergan (Promethazine)E100% (1)
- AMINOPHYLLINEДокумент2 страницыAMINOPHYLLINEmusiclover017100% (1)
- Case Pre Drug StudyДокумент5 страницCase Pre Drug StudyJoule PeirreОценок пока нет
- Valproic AcidДокумент4 страницыValproic Acidapi-3797941100% (2)
- Miglitol (Glyset)Документ1 страницаMiglitol (Glyset)EОценок пока нет
- Duty Drug Study'sДокумент7 страницDuty Drug Study'sGrape JuiceОценок пока нет
- DrugДокумент4 страницыDrugVANNEZA TRIXZY TAMPARONGОценок пока нет
- Lyrica Drug StudyДокумент3 страницыLyrica Drug StudydyndzОценок пока нет
- SimethiconeДокумент1 страницаSimethiconeDivine Dela PenaОценок пока нет
- AlprazolamДокумент3 страницыAlprazolamapi-3797941100% (1)
- AcetazolamideДокумент2 страницыAcetazolamideLIEZEL GRACE VELAYOОценок пока нет
- DRug Study PhenytoinДокумент1 страницаDRug Study Phenytoinmichelle marquezОценок пока нет
- Drug Study Table 3Документ5 страницDrug Study Table 3Juliet De GuzmanОценок пока нет
- Drug - Htm#description.: Reference: Submitted By: Date Submitted: Submitted ToДокумент2 страницыDrug - Htm#description.: Reference: Submitted By: Date Submitted: Submitted ToSHEILA MAE SACLOTОценок пока нет
- Chloral Hydrate (Drug Study)Документ3 страницыChloral Hydrate (Drug Study)Franz.thenurse6888Оценок пока нет
- Formoterol Gonzaga.Документ2 страницыFormoterol Gonzaga.Sheryl Anne GonzagaОценок пока нет
- Carbidopa Levodopa SinemetДокумент3 страницыCarbidopa Levodopa SinemetTodd ColeОценок пока нет
- Ditropan Drug CardДокумент2 страницыDitropan Drug CardBenОценок пока нет
- Magnesium Sulfate Drug StudyДокумент3 страницыMagnesium Sulfate Drug StudyMonica Lyka BancaleОценок пока нет
- AminophyllineДокумент9 страницAminophyllineZaira BataloОценок пока нет
- Generic Name: Brand Name:: ClassificationsДокумент2 страницыGeneric Name: Brand Name:: ClassificationsbillyktoubattsОценок пока нет
- Labetalol Hydro ChlorideДокумент3 страницыLabetalol Hydro Chlorideapi-3797941100% (1)
- PiroxicamДокумент2 страницыPiroxicamVirginia Aira Lara MarquezОценок пока нет
- GlipizideДокумент2 страницыGlipizideFeliciaDorghamОценок пока нет
- BisoprololДокумент2 страницыBisoprololNovi YulianaОценок пока нет
- Hydralazine.1 3Документ1 страницаHydralazine.1 3SОценок пока нет
- AmlodipineДокумент2 страницыAmlodipineAnonymous QqyLDoW1Оценок пока нет
- Med Surg Medication Study GuideДокумент8 страницMed Surg Medication Study Guidetina100% (1)
- Drug StudyДокумент33 страницыDrug Studyjefwy8Оценок пока нет
- CaptoprilДокумент3 страницыCaptoprilNovi YulianaОценок пока нет
- BisoprololДокумент2 страницыBisoprololNovi YulianaОценок пока нет
- NifedipineДокумент3 страницыNifedipineNovi YulianaОценок пока нет
- RamiprilДокумент3 страницыRamiprilNovi YulianaОценок пока нет
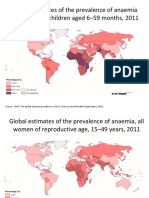
- Global Estimates of The Prevalence of Anaemia in Infants and Children Aged 6 59 Months, 2011Документ4 страницыGlobal Estimates of The Prevalence of Anaemia in Infants and Children Aged 6 59 Months, 2011Novi YulianaОценок пока нет
- Infectious Agents and Cancer: Antiviral Therapy in Acute Viral Hepatitis B: Why and WhenДокумент2 страницыInfectious Agents and Cancer: Antiviral Therapy in Acute Viral Hepatitis B: Why and WhenNovi YulianaОценок пока нет
- Farmakoterapi Coagulation DisorderДокумент55 страницFarmakoterapi Coagulation DisorderNur Astuty PurnamasariОценок пока нет
- WA Health Consent To Treatment Policy: Better Health Better Care Better ValueДокумент42 страницыWA Health Consent To Treatment Policy: Better Health Better Care Better ValueprabhaОценок пока нет
- Chemistry ProjectДокумент13 страницChemistry ProjectPranjal GiriОценок пока нет
- Toc PDFДокумент12 страницToc PDFraviraja moduguОценок пока нет
- Evaluation of Tablet PDFДокумент2 страницыEvaluation of Tablet PDFKim50% (2)
- Cirrhosis and Its Complications Evidence Based TreatmentДокумент20 страницCirrhosis and Its Complications Evidence Based TreatmentSucii Sekar NingrumОценок пока нет
- Howtousea Nebulizer in Pediatric ClientsДокумент11 страницHowtousea Nebulizer in Pediatric ClientsAngelina Nicole G. TungolОценок пока нет
- Efficacy of Ethanol Against Viruses in Hand DisinfectionДокумент9 страницEfficacy of Ethanol Against Viruses in Hand DisinfectionImaec LimitedОценок пока нет
- DR Craig WeilДокумент14 страницDR Craig WeilPaula OwensОценок пока нет
- NCP Deficit Fluid VolumeДокумент4 страницыNCP Deficit Fluid VolumeKingJayson Pacman06Оценок пока нет
- LAP DirectoryДокумент36 страницLAP Directorydolly wattaОценок пока нет
- ORAL CANCER - Edited by Kalu U. E. OgburekeДокумент400 страницORAL CANCER - Edited by Kalu U. E. Ogburekeعبد المنعم مصباحيОценок пока нет
- SyphilisДокумент54 страницыSyphilisYeyeh SantosОценок пока нет
- The Therapy BookДокумент398 страницThe Therapy BookAbdelrahman Mamdouh90% (10)
- Hypovolemic Shock Concept MapДокумент1 страницаHypovolemic Shock Concept MapJM AsentistaОценок пока нет
- Case PresДокумент22 страницыCase Presandrei jinОценок пока нет
- 136 AДокумент5 страниц136 AMarcelitaTaliaDuwiriОценок пока нет
- PHARMEVOДокумент3 страницыPHARMEVOFariha AnsariОценок пока нет
- Chorionic Bump in First-Trimester Sonography: SciencedirectДокумент6 страницChorionic Bump in First-Trimester Sonography: SciencedirectEdward EdwardОценок пока нет
- DR Adedayo OSHOLOWU - Clinical Director - Special Olympics - NIGERIAДокумент3 страницыDR Adedayo OSHOLOWU - Clinical Director - Special Olympics - NIGERIAAdedayo OsholowuОценок пока нет
- Neolus: Single Use Hypodermic NeedlesДокумент2 страницыNeolus: Single Use Hypodermic Needlesmiumau3Оценок пока нет
- Pathophysiology of Acute GastroenteritisДокумент5 страницPathophysiology of Acute Gastroenteritisheron_bayanin_15Оценок пока нет
- Importance and Purposes of ResearchДокумент3 страницыImportance and Purposes of ResearchKarl Kiw-isОценок пока нет
- Sandra John - Case Scenario On Bulimia NervosaДокумент7 страницSandra John - Case Scenario On Bulimia Nervosasandra0% (1)
- ACUTE ABDOMEN Systemic SonographicДокумент6 страницACUTE ABDOMEN Systemic SonographiciwanОценок пока нет
- Medsave - Claim Form For MediclaimДокумент1 страницаMedsave - Claim Form For Mediclaimpawan1501Оценок пока нет
- Revie Jurnal Sources of Stress and Coping StrategiesДокумент7 страницRevie Jurnal Sources of Stress and Coping StrategiesAmieОценок пока нет
- Rash Diagnosis Cheat Sheet: EmergencyДокумент1 страницаRash Diagnosis Cheat Sheet: Emergencykdlsfk kajjksolsОценок пока нет
- 2023 Music Therapy & NICUДокумент36 страниц2023 Music Therapy & NICUMohammad Izaan TahirОценок пока нет