Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Letter of Late EnrollmentДокумент1 страницаLetter of Late EnrollmentRomi Necq S. Abuel50% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Rules & Regulations Governing Fraternities & Sororities - 0Документ8 страницRules & Regulations Governing Fraternities & Sororities - 0Romi Necq S. AbuelОценок пока нет
- Rules & Regulations Governing Fraternities & Sororities - 0Документ8 страницRules & Regulations Governing Fraternities & Sororities - 0Romi Necq S. AbuelОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- AP191 1st Problem SetДокумент2 страницыAP191 1st Problem SetRomi Necq S. AbuelОценок пока нет
- Republic Act No 8049 PDFДокумент3 страницыRepublic Act No 8049 PDFRomi Necq S. AbuelОценок пока нет
- Buhay Frat PSP PsuДокумент21 страницаBuhay Frat PSP PsuRomi Necq S. AbuelОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Circuit Simulation PDFДокумент4 страницыCircuit Simulation PDFRomi Necq S. AbuelОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- PE 2 Badminton Syllabus UP ManilaДокумент2 страницыPE 2 Badminton Syllabus UP ManilaRomi Necq S. Abuel67% (3)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Cinema Rehiyon 7 HighResДокумент89 страницCinema Rehiyon 7 HighResRomi Necq S. AbuelОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Circuit Simulation Using Symetrix/SIMPLISДокумент4 страницыCircuit Simulation Using Symetrix/SIMPLISRomi Necq S. AbuelОценок пока нет
- Three Lectures On History and PhasesДокумент4 страницыThree Lectures On History and PhasesRomi Necq S. AbuelОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
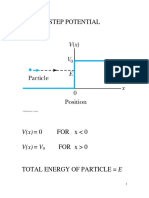
- Step Potential PDFДокумент34 страницыStep Potential PDFRomi Necq S. AbuelОценок пока нет
- Example of Lab ReportДокумент6 страницExample of Lab ReportRomi Necq S. AbuelОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Bio 22 Lab Cell Transport ExperimentДокумент6 страницBio 22 Lab Cell Transport ExperimentRomi Necq S. Abuel100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
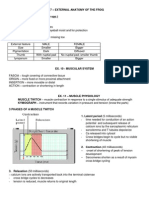
- Bio 22 - Exercise 11 and 13 - Muscle Physiology and Nervous Response NotesДокумент4 страницыBio 22 - Exercise 11 and 13 - Muscle Physiology and Nervous Response NotesRomi Necq S. AbuelОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Physics 71 Rotation Problem Set: 1 CollisionsДокумент3 страницыPhysics 71 Rotation Problem Set: 1 CollisionsRomi Necq S. AbuelОценок пока нет
- Effect of Technology On Learning and Development of StudentsДокумент3 страницыEffect of Technology On Learning and Development of StudentsRomi Necq S. AbuelОценок пока нет
- Tragedy of The CommonsДокумент2 страницыTragedy of The CommonsRomi Necq S. AbuelОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Chem. 14.1 - Expt. 9 Chem Lab Report - Chemical EquilibriumДокумент3 страницыChem. 14.1 - Expt. 9 Chem Lab Report - Chemical EquilibriumRomi Necq S. Abuel40% (5)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Philippine Historical Emergent PhaseДокумент13 страницPhilippine Historical Emergent PhaseRomi Necq S. AbuelОценок пока нет
- Political Science - Social Science 1 UPMДокумент25 страницPolitical Science - Social Science 1 UPMRomi Necq S. AbuelОценок пока нет
- Math 17 First Exam 2013 UPMДокумент2 страницыMath 17 First Exam 2013 UPMRomi Necq S. AbuelОценок пока нет
- Open FracturesДокумент51 страницаOpen FracturesStar Cruise100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Pedia Notes PrintДокумент6 страницPedia Notes PrintDre Valdez100% (5)
- Instruction For Author ClimactericДокумент9 страницInstruction For Author ClimactericAndi BintangОценок пока нет
- Huether: Understanding Pathophysiology, 6th EditionДокумент4 страницыHuether: Understanding Pathophysiology, 6th EditionTecsh DeckgirlОценок пока нет
- Rebt Vs CT Vs Med in DepressionДокумент19 страницRebt Vs CT Vs Med in DepressionPaula StroianОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Catatonia PDFДокумент9 страницCatatonia PDFDanilo RibeiroОценок пока нет
- Drug StudyДокумент14 страницDrug StudyRaff GutierrezОценок пока нет
- WHO MC - Manual - 2018 PDFДокумент403 страницыWHO MC - Manual - 2018 PDFchimbimbОценок пока нет
- DR I ClementДокумент21 страницаDR I ClementDR.I.CLEMENT50% (2)
- Guideline HEGДокумент5 страницGuideline HEGMushlihani HaniОценок пока нет
- 2 02-Electrocardiography PDFДокумент17 страниц2 02-Electrocardiography PDFMiguel DomingoОценок пока нет
- Hospital Standards For Accreditation For Afghanistan Hosp - Standards - PharmacyДокумент10 страницHospital Standards For Accreditation For Afghanistan Hosp - Standards - PharmacyMaria Camila100% (1)
- Arthrogryposis Multiplex Congenita of The Upper Limb: Linical RticleДокумент6 страницArthrogryposis Multiplex Congenita of The Upper Limb: Linical RticleBlajiu BeatriceОценок пока нет
- Perception DisordersДокумент4 страницыPerception DisordersSabi HassanОценок пока нет
- 2011 MicrogynonДокумент16 страниц2011 MicrogynontaikucinglohОценок пока нет
- 10-Effect of Chest Physical Therapy On Pediatrics Hospitalized With Pneumonia PDFДокумент8 страниц10-Effect of Chest Physical Therapy On Pediatrics Hospitalized With Pneumonia PDFandina100% (1)
- Vascular Note by Joel ArudchelvamДокумент52 страницыVascular Note by Joel ArudchelvamJoel Arudchelvam100% (1)
- Necrotizing Facitis ReviewДокумент16 страницNecrotizing Facitis ReviewHadi Firmansyah SidiqОценок пока нет
- Definition of Osteoporosis: Symptoms of OsteoporosisДокумент3 страницыDefinition of Osteoporosis: Symptoms of OsteoporosisYing Flavia100% (2)
- Thalassemia BrochureДокумент4 страницыThalassemia Brochurevein94Оценок пока нет
- Post-Mortem ExaminationДокумент7 страницPost-Mortem ExaminationLeninRickyОценок пока нет
- First Aid JeopardyДокумент52 страницыFirst Aid Jeopardyfable32Оценок пока нет
- HCVДокумент33 страницыHCVsherif555Оценок пока нет
- What Is HyperthymesiaДокумент2 страницыWhat Is HyperthymesiaCarlos BellatinОценок пока нет
- Euros Core OrgДокумент6 страницEuros Core OrgClaudio Walter VidelaОценок пока нет
- Private Practice in Ophthalmology: - Making It WorkДокумент16 страницPrivate Practice in Ophthalmology: - Making It WorkFuadОценок пока нет
- Tactical Casualty Combat Care Handbook v5 PDFДокумент133 страницыTactical Casualty Combat Care Handbook v5 PDFJose Torres100% (5)
- Management of Severe Hyperkalemia PDFДокумент6 страницManagement of Severe Hyperkalemia PDFCarlos Navarro YslaОценок пока нет
- K Burns Qualitative Research PosterДокумент1 страницаK Burns Qualitative Research Posterapi-257576036Оценок пока нет
- Meningitis-Malaria E PDFДокумент44 страницыMeningitis-Malaria E PDFSana ShafeeqОценок пока нет