Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Cerebral Palsy Assessment ImportantДокумент7 страницCerebral Palsy Assessment Importantabra_arr100% (2)
- Physioex Lab Report: Pre-Lab Quiz ResultsДокумент4 страницыPhysioex Lab Report: Pre-Lab Quiz ResultsNovanza RayhanОценок пока нет
- Ndeb Released Question Bank - 2017Документ464 страницыNdeb Released Question Bank - 2017Basant Shams80% (20)
- Mcqs PhysiologyДокумент96 страницMcqs PhysiologyKandiwapaОценок пока нет
- Sanctification of The Heart 4th Edition by DR Michelle StrydomДокумент771 страницаSanctification of The Heart 4th Edition by DR Michelle StrydomDios Estrella67% (3)
- Total Leukocyte Count by HemocytometerДокумент4 страницыTotal Leukocyte Count by HemocytometerMalkish RajkumarОценок пока нет
- Understanding-Ocd 2016 v2Документ27 страницUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- Basic Implant SurgeryДокумент72 страницыBasic Implant SurgeryKandiwapa100% (2)
- Advanced Burn Life SupportДокумент118 страницAdvanced Burn Life SupportIntan Noa100% (1)
- 4 5809670530357265615 PDFДокумент420 страниц4 5809670530357265615 PDFOmar SiddigОценок пока нет
- Pre-Test Maternal and Child Health NursingДокумент18 страницPre-Test Maternal and Child Health NursingDefensor Pison GringgoОценок пока нет
- Casebook 2007Документ209 страницCasebook 2007KandiwapaОценок пока нет
- BDA Consent 2016Документ9 страницBDA Consent 2016KandiwapaОценок пока нет
- Degenerative Disorders of The Temporomandibular Joint: Etiology, Diagnosis, and TreatmentДокумент13 страницDegenerative Disorders of The Temporomandibular Joint: Etiology, Diagnosis, and TreatmentKandiwapaОценок пока нет
- Recurrent Aphtous StomatitisДокумент34 страницыRecurrent Aphtous StomatitisKandiwapaОценок пока нет
- Topic.11 Teeth Discoloration and BleachingДокумент7 страницTopic.11 Teeth Discoloration and BleachingKandiwapaОценок пока нет
- Topic 3 Dental DepositsДокумент5 страницTopic 3 Dental DepositsKandiwapaОценок пока нет
- Children's dental health: Retention of teethДокумент4 страницыChildren's dental health: Retention of teethKandiwapaОценок пока нет
- Oral Manifestations of TuberculosisДокумент4 страницыOral Manifestations of TuberculosisKandiwapaОценок пока нет
- Acute Necrotizing Ulcerative Gingivitis Copy 2Документ3 страницыAcute Necrotizing Ulcerative Gingivitis Copy 2KandiwapaОценок пока нет
- Cardiology Case 1Документ2 страницыCardiology Case 1vil62650% (2)
- Aula 1Документ14 страницAula 1Brigida Cirqueira GuimaraesОценок пока нет
- QuestionsДокумент6 страницQuestionsLorvic Andrew Juanson UmaliОценок пока нет
- Hypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentДокумент11 страницHypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentAnantaBenvenutoОценок пока нет
- Source Control in Emergency General SurgeryДокумент21 страницаSource Control in Emergency General SurgerylaviniaОценок пока нет
- Conscious Sedation PaediatricsДокумент44 страницыConscious Sedation PaediatricsReeta TaxakОценок пока нет
- HEPATITIS B VACCINE NURSING RESPONSIBILITIESДокумент14 страницHEPATITIS B VACCINE NURSING RESPONSIBILITIESJannine BensiОценок пока нет
- IV Drug ReactionsДокумент19 страницIV Drug Reactionsphp_czarina04421Оценок пока нет
- Basic pharmacology of anaesthesia drugs in 40 charactersДокумент56 страницBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87Оценок пока нет
- NobelReplace Conical Connect OverviewДокумент6 страницNobelReplace Conical Connect Overviewaziz2007Оценок пока нет
- Remote Area Nursing Emergency GuidelinesДокумент325 страницRemote Area Nursing Emergency Guidelineslavinia_dobrescu_1Оценок пока нет
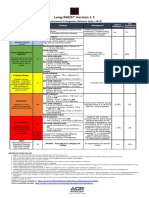
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Документ1 страницаLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotОценок пока нет
- Week 29 - DRRRДокумент5 страницWeek 29 - DRRRMira VeranoОценок пока нет
- Definition:: Between 16Документ3 страницыDefinition:: Between 16NIDA MUSTAFAОценок пока нет
- Route To: Nnovative Joints Ejuvenation CentreДокумент2 страницыRoute To: Nnovative Joints Ejuvenation CentreAnil Kumar.VОценок пока нет
- Safe SexДокумент11 страницSafe SexnathanОценок пока нет
- Milobar Alexus Resume MayoДокумент2 страницыMilobar Alexus Resume Mayoapi-338646789Оценок пока нет
- Fetal risks of macrosomia in diabetic pregnanciesДокумент27 страницFetal risks of macrosomia in diabetic pregnanciesIful SaifullahОценок пока нет
- Final Written Lab Exam Form AДокумент4 страницыFinal Written Lab Exam Form AErvin T MileОценок пока нет
- Role of Autologous Platelet-Rich Plasma in Z-PlastyДокумент3 страницыRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsОценок пока нет
- Hipertensi Portal Donny SandraДокумент67 страницHipertensi Portal Donny SandrabobyОценок пока нет
- ShineДокумент37 страницShineMohd SaifОценок пока нет
- Literature Review Type 2 DiabetesДокумент4 страницыLiterature Review Type 2 Diabetesafmaadalrefplh100% (1)