Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Solutions To Irodov's Problems - Volume IIДокумент442 страницыSolutions To Irodov's Problems - Volume IIZequinha de Abreu100% (2)
- Silo Cement CalculationДокумент11 страницSilo Cement CalculationFikriaraz AfifОценок пока нет
- Oracle Data Integration - An Overview With Emphasis in DW AppДокумент34 страницыOracle Data Integration - An Overview With Emphasis in DW Appkinan_kazuki104Оценок пока нет
- Mitsubishi diesel forklifts 1.5-3.5 tonnesДокумент2 страницыMitsubishi diesel forklifts 1.5-3.5 tonnesJoniОценок пока нет
- Disclosure To Promote The Right To InformationДокумент22 страницыDisclosure To Promote The Right To InformationJGD123Оценок пока нет
- CaselogsДокумент2 страницыCaselogsapi-337185638Оценок пока нет
- Final DraftДокумент15 страницFinal Draftapi-334402872Оценок пока нет
- CaselogsДокумент2 страницыCaselogsapi-337185638Оценок пока нет
- Csi Sheil FinalДокумент12 страницCsi Sheil Finalapi-337185638Оценок пока нет
- Practice Problems Weeks 1 2 For StudentsДокумент1 страницаPractice Problems Weeks 1 2 For Studentsapi-337168367Оценок пока нет
- Volunteer - AamdДокумент3 страницыVolunteer - Aamdapi-337185638Оценок пока нет
- Fall Eval 1Документ3 страницыFall Eval 1api-337185638Оценок пока нет
- Fall Eval 1Документ3 страницыFall Eval 1api-337185638Оценок пока нет
- Fall Eval 2Документ3 страницыFall Eval 2api-337185638Оценок пока нет
- Eval 2nd Semester - 2Документ3 страницыEval 2nd Semester - 2api-337185638Оценок пока нет
- Safetypaper SheilДокумент4 страницыSafetypaper Sheilapi-337185638Оценок пока нет
- Leipzig Cone ApplicatorsДокумент2 страницыLeipzig Cone Applicatorsapi-337185638Оценок пока нет
- Final DraftДокумент18 страницFinal Draftapi-334402872Оценок пока нет
- Final Qa TablesДокумент10 страницFinal Qa Tablesapi-337185638Оценок пока нет
- Eval 2nd Semester-1Документ3 страницыEval 2nd Semester-1api-337185638Оценок пока нет
- CaselogsДокумент2 страницыCaselogsapi-337185638Оценок пока нет
- Sheil ServicelearningДокумент4 страницыSheil Servicelearningapi-337185638Оценок пока нет
- Vaginal CylinderДокумент2 страницыVaginal Cylinderapi-337185638Оценок пока нет
- Sheil ServicelearningДокумент4 страницыSheil Servicelearningapi-337185638Оценок пока нет
- Clinicaleval Firstsemester1Документ3 страницыClinicaleval Firstsemester1api-337185638Оценок пока нет
- Volunteer - AamdДокумент3 страницыVolunteer - Aamdapi-337185638Оценок пока нет
- The Computer SystemДокумент1 страницаThe Computer Systemapi-337185638Оценок пока нет
- CaselogsДокумент2 страницыCaselogsapi-337185638Оценок пока нет
- Comparative Article-2Документ8 страницComparative Article-2api-337185638Оценок пока нет
- Standard Uptake ValueДокумент2 страницыStandard Uptake Valueapi-337185638Оценок пока нет
- Sheil TreatmentplanningprojectДокумент11 страницSheil Treatmentplanningprojectapi-337185638Оценок пока нет
- Aprilcasestudy Sheil-4Документ17 страницAprilcasestudy Sheil-4api-337185638Оценок пока нет
- Pelvis Lab Sheil-1Документ12 страницPelvis Lab Sheil-1api-337185638Оценок пока нет
- Sheil Lunglab-2Документ10 страницSheil Lunglab-2api-337185638Оценок пока нет
- CI SetДокумент18 страницCI Setতন্ময় ঢালি Tanmay DhaliОценок пока нет
- Biogen 2021Документ12 страницBiogen 2021taufiq hidОценок пока нет
- Chapter 11 revision notes on budgeting and planningДокумент5 страницChapter 11 revision notes on budgeting and planningRoli YonoОценок пока нет
- Leroy Somer 3434c - GB-NyДокумент28 страницLeroy Somer 3434c - GB-NyCris_eu09100% (1)
- PDF Solution Manual For Gas Turbine Theory 6th Edition Saravanamuttoo Rogers CompressДокумент7 страницPDF Solution Manual For Gas Turbine Theory 6th Edition Saravanamuttoo Rogers CompressErickson Brayner MarBerОценок пока нет
- Answer Key Grade 6 - 2023Документ7 страницAnswer Key Grade 6 - 2023ALKHANSAA ELOBEIDYОценок пока нет
- Satellite TestingДокумент30 страницSatellite TestingXavier Ponce Ferrufino100% (1)
- 02-OceanStor Dorado 3 Highlights and 9 Must-Know Points 1.0Документ5 страниц02-OceanStor Dorado 3 Highlights and 9 Must-Know Points 1.0QQОценок пока нет
- Regeln Map 2Документ2 страницыRegeln Map 2bruno.wetzelОценок пока нет
- 4495 10088 1 PBДокумент7 страниц4495 10088 1 PBGeorgius Kent DiantoroОценок пока нет
- College of Information Technology Dmmmsu-Mluc City of San FernandoДокумент9 страницCollege of Information Technology Dmmmsu-Mluc City of San FernandoZoilo BagtangОценок пока нет
- Jaguar Land Rover Configuration Lifecycle Management WebДокумент4 страницыJaguar Land Rover Configuration Lifecycle Management WebStar Nair Rock0% (1)
- Turbine Buyers Guide - Mick Sagrillo & Ian WoofendenДокумент7 страницTurbine Buyers Guide - Mick Sagrillo & Ian WoofendenAnonymous xYhjeilnZОценок пока нет
- Valve Actuator Data SheetДокумент1 страницаValve Actuator Data SheetRob StorrowОценок пока нет
- SPPID QuestionsДокумент2 страницыSPPID Questionsvivek83% (12)
- Craig Vaughan CHPTR 07Документ44 страницыCraig Vaughan CHPTR 07Jorge CananeaОценок пока нет
- Unit 10Документ18 страницUnit 10ChaithraMalluОценок пока нет
- GenEd Mathematics LLL PDFДокумент32 страницыGenEd Mathematics LLL PDFArmely NiedoОценок пока нет
- Astm D5501Документ3 страницыAstm D5501mhmdgalalОценок пока нет
- PresiometroДокумент25 страницPresiometrojoseprepaОценок пока нет
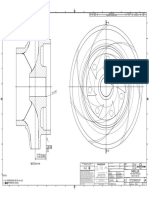
- Impeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLДокумент1 страницаImpeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLSenthilkumar RamalingamОценок пока нет
- 08 Candelaria Punta Del Cobre IOCG Deposits PDFДокумент27 страниц08 Candelaria Punta Del Cobre IOCG Deposits PDFDiego Morales DíazОценок пока нет
- Design of Shaft Straightening MachineДокумент58 страницDesign of Shaft Straightening MachineChiragPhadkeОценок пока нет
- 2.6 Rational Functions Asymptotes TutorialДокумент30 страниц2.6 Rational Functions Asymptotes TutorialAljun Aldava BadeОценок пока нет
- F (X, Y) Sin (Xy) + X LN (Y) Find F at (0, )Документ9 страницF (X, Y) Sin (Xy) + X LN (Y) Find F at (0, )muhammad abrarОценок пока нет