Вам также может понравиться
- Sample Preschool Registration FormДокумент4 страницыSample Preschool Registration FormSir CalaqueiОценок пока нет
- Emma - Schofield@parliament - Uk: Re: Your Complaint Regarding My DentistДокумент3 страницыEmma - Schofield@parliament - Uk: Re: Your Complaint Regarding My DentistTОценок пока нет
- Preschool Registration: 2011-2012: Age Cost FrequencyДокумент8 страницPreschool Registration: 2011-2012: Age Cost FrequencyNewLifePreschoolОценок пока нет
- Enrollement Form Day Care 1Документ3 страницыEnrollement Form Day Care 1fatimahjawwad9697Оценок пока нет
- Registration Form FebruaryДокумент11 страницRegistration Form Februaryapi-279262001Оценок пока нет
- 2017 Camp RegistrationДокумент5 страниц2017 Camp RegistrationmcmurraycОценок пока нет
- Universal Credit Work Capability QuestionnaireДокумент24 страницыUniversal Credit Work Capability QuestionnaireSteven Preece100% (2)
- 2011 Camp Application 2Документ3 страницы2011 Camp Application 2Amanda ReedОценок пока нет
- Children S Services Referral FormДокумент4 страницыChildren S Services Referral FormChinggay CuarterosОценок пока нет
- Application Form 2018Документ3 страницыApplication Form 2018api-282461840Оценок пока нет
- Child Data SheetДокумент2 страницыChild Data SheetthemaninthemoonОценок пока нет
- CBC 2013 WaiverandRelease Minor FormДокумент1 страницаCBC 2013 WaiverandRelease Minor FormCory James HutchersonОценок пока нет
- Emergency Information FormДокумент2 страницыEmergency Information FormGrace Lutheran SandyОценок пока нет
- Morning ProgramДокумент5 страницMorning ProgramOrtizОценок пока нет
- 2013-Appendix-2 1-Child-Enrolment-FormДокумент15 страниц2013-Appendix-2 1-Child-Enrolment-Formapi-311470786Оценок пока нет
- Emergency Contact Form AthleticsДокумент2 страницыEmergency Contact Form AthleticsJeremiah HartyОценок пока нет
- Enrolment Form 2022 2023Документ6 страницEnrolment Form 2022 2023jarrad agiusОценок пока нет
- Child and Adolescent History Form: Rappahannock Area Community Services BoardДокумент14 страницChild and Adolescent History Form: Rappahannock Area Community Services BoardSanziana SavaОценок пока нет
- Child Information SheetДокумент2 страницыChild Information SheetElizabeth Degen-SkillingОценок пока нет
- DS700 Carer Alllowance Claim FormДокумент28 страницDS700 Carer Alllowance Claim FormHassan Mussa KhamisОценок пока нет
- Midrand Montessori Preschool EnrolmentДокумент8 страницMidrand Montessori Preschool Enrolmentanarki85Оценок пока нет
- Letter + Litigation PacketДокумент16 страницLetter + Litigation PacketJames HumphreysОценок пока нет
- Maternal Child Home Visiting ReferralДокумент2 страницыMaternal Child Home Visiting ReferralNurlatifah FebrianaОценок пока нет
- Patient Data SheetДокумент2 страницыPatient Data SheetArgel Hanzon NietesОценок пока нет
- Abcd Early Learning Application Packet: Office Use OnlyДокумент11 страницAbcd Early Learning Application Packet: Office Use OnlyrockyОценок пока нет
- SAMPLE Complaint LetterДокумент2 страницыSAMPLE Complaint Letterjacs79Оценок пока нет
- Neo Registration Forms AДокумент4 страницыNeo Registration Forms Aapi-247079386Оценок пока нет
- Ymca Camp Permission & Health Form: Additional Authorized Persons For Pick UpДокумент4 страницыYmca Camp Permission & Health Form: Additional Authorized Persons For Pick Upahcobras1314Оценок пока нет
- Custody and Parenting Time QuestionnaireДокумент6 страницCustody and Parenting Time QuestionnaireStephanie WilsonОценок пока нет
- Contract Sheet1Документ1 страницаContract Sheet1api-233310437Оценок пока нет
- One Copy of Your Current Heating Bill Proof of The Past 3 Full Months of Gross For Social Security or Va You Must Send AДокумент8 страницOne Copy of Your Current Heating Bill Proof of The Past 3 Full Months of Gross For Social Security or Va You Must Send ASusan GoettschОценок пока нет
- ChildrensenrollmentДокумент3 страницыChildrensenrollmentapi-254198210Оценок пока нет
- 4 Yeldall Application Form PrintableДокумент10 страниц4 Yeldall Application Form Printableapi-634298404Оценок пока нет
- CAS Application Form 2021-22 English FINAL PDFДокумент3 страницыCAS Application Form 2021-22 English FINAL PDFMichael O Connor0% (1)
- Pediatric Patient Registration Form TemplateДокумент5 страницPediatric Patient Registration Form TemplateHasfi YakobОценок пока нет
- New Patient FormДокумент4 страницыNew Patient Formapi-288684181Оценок пока нет
- Lincoln Lutheran Student Profile FormДокумент4 страницыLincoln Lutheran Student Profile FormSalmaОценок пока нет
- Airport High School Band 2009-2010 Student Health History andДокумент1 страницаAirport High School Band 2009-2010 Student Health History andapi-12924807Оценок пока нет
- Primary To Secondary 2015Документ4 страницыPrimary To Secondary 2015ifyoutickleusОценок пока нет
- Parental ConsentДокумент2 страницыParental Consentapi-319115928Оценок пока нет
- Client Intake Form: (Last) (First) (MI)Документ20 страницClient Intake Form: (Last) (First) (MI)Prabha Gupta0% (1)
- Ascension Macomb Oakland Hospital Volunteer ApplicationДокумент5 страницAscension Macomb Oakland Hospital Volunteer ApplicationRodney DaliegeОценок пока нет
- ECE 3 Year Old: 2012-2013 School Year (Round 2) : Student InformationДокумент5 страницECE 3 Year Old: 2012-2013 School Year (Round 2) : Student Information007003sОценок пока нет
- Emergency Medical FormДокумент1 страницаEmergency Medical FormDarren MorrisonОценок пока нет
- Application Form EnglishДокумент2 страницыApplication Form EnglishMACENZIE WAKEFIELD0% (1)
- Babysitter Consent and Contact FormДокумент2 страницыBabysitter Consent and Contact Form2mvpОценок пока нет
- Nursing Admission FormДокумент6 страницNursing Admission FormErdin TriansyahОценок пока нет
- Specialist Assessment Service Referral Form September 2017Документ14 страницSpecialist Assessment Service Referral Form September 2017Rebecca CurranОценок пока нет
- ObjectionДокумент5 страницObjectionJohn Tyberious SmithОценок пока нет
- Welcome Rev2Документ2 страницыWelcome Rev2Adam C. Price100% (1)
- NEW Registration Form April 2022Документ4 страницыNEW Registration Form April 2022Kraftworks AcademyОценок пока нет
- Private & Confidential Miss V Livadari 24A Southend Lane London Se6 3aaДокумент11 страницPrivate & Confidential Miss V Livadari 24A Southend Lane London Se6 3aaIon LozovanuОценок пока нет
- 2011 General Student Information Form 1 FORMATTEDДокумент2 страницы2011 General Student Information Form 1 FORMATTEDBuen SaliganОценок пока нет
- Senior Conference 2013 FormsДокумент7 страницSenior Conference 2013 FormsshamswayОценок пока нет
- New Contract14Документ2 страницыNew Contract14api-232676731Оценок пока нет
- Name - Camp Kesem Camper Application General InformationДокумент6 страницName - Camp Kesem Camper Application General InformationSarah AxelrodОценок пока нет
- Complaint Letter Template for Unsatisfactory Medical ServiceДокумент4 страницыComplaint Letter Template for Unsatisfactory Medical ServiceZdenka PetroskyОценок пока нет
- RRДокумент2 страницыRRaliОценок пока нет
- NAWARA Pipeline QC Team Handover: Dorri Hriz With Ahmed Rekhis On Saturday 09/12/2017Документ1 страницаNAWARA Pipeline QC Team Handover: Dorri Hriz With Ahmed Rekhis On Saturday 09/12/2017aliОценок пока нет
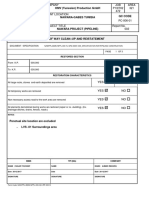
- Pipe Handover ReportДокумент1 страницаPipe Handover ReportaliОценок пока нет
- C5+ As Built TableДокумент19 страницC5+ As Built TablealiОценок пока нет
- I Couldn't Help It !!!: ConversationДокумент13 страницI Couldn't Help It !!!: ConversationaliОценок пока нет
- Sample LettersДокумент8 страницSample LettersaliОценок пока нет
- Nawara Pipeline Project Nawara Pipeline Project: Milestones MilestonesДокумент11 страницNawara Pipeline Project Nawara Pipeline Project: Milestones Milestonesali100% (1)
- 0002Документ1 страница0002aliОценок пока нет
- Scketch ReportДокумент2 страницыScketch ReportaliОценок пока нет
- ReinstatementДокумент3 страницыReinstatementaliОценок пока нет
- RRДокумент2 страницыRRaliОценок пока нет
- Scketch ReportДокумент3 страницыScketch ReportaliОценок пока нет
- New Text DocumentДокумент1 страницаNew Text DocumentaliОценок пока нет
- AweetДокумент1 страницаAweetaliОценок пока нет
- Cccam Soft4satДокумент7 страницCccam Soft4sataliОценок пока нет
- AweetДокумент1 страницаAweetaliОценок пока нет
- AliwuuixxuuuxДокумент1 страницаAliwuuixxuuuxdddddddОценок пока нет
- AliwuuixxuuuxДокумент1 страницаAliwuuixxuuuxdddddddОценок пока нет
- 4th QUARTER EXAMINATION IN TLE 8Документ3 страницы4th QUARTER EXAMINATION IN TLE 8judy ann sottoОценок пока нет
- 1.4 Market FailureДокумент42 страницы1.4 Market FailureRuban PaulОценок пока нет
- QIMA - Ethical Audit Preparation Document - ENДокумент3 страницыQIMA - Ethical Audit Preparation Document - ENMD Nurul HudaОценок пока нет
- Strain Gauge Load Cells LPB0005IДокумент2 страницыStrain Gauge Load Cells LPB0005ILordbyron23Оценок пока нет
- Mini City Direct Heating SubstationДокумент4 страницыMini City Direct Heating SubstationPaul ButucОценок пока нет
- Reglas para Añadir Al Verbo Principal: Am Is Are ReadДокумент8 страницReglas para Añadir Al Verbo Principal: Am Is Are ReadBrandon Sneider Garcia AriasОценок пока нет
- Children's Test Anxiety Scale (CTASДокумент10 страницChildren's Test Anxiety Scale (CTASSchahyda ArleyОценок пока нет
- Epreuve LV 2 Anglais Premiere L Composition 2e Semestre 2023Документ2 страницыEpreuve LV 2 Anglais Premiere L Composition 2e Semestre 2023Thierno ousmane DialloОценок пока нет
- Fabrication and Installation of Vertical Steel Pressure ShaftДокумент23 страницыFabrication and Installation of Vertical Steel Pressure ShaftPasan RajasingheОценок пока нет
- The Design of The 2016-17 Young Lives School Survey in EthiopiaДокумент10 страницThe Design of The 2016-17 Young Lives School Survey in EthiopiaFuadОценок пока нет
- 2 - Electrical Energy Audit PDFДокумент10 страниц2 - Electrical Energy Audit PDFPrachi BhaveОценок пока нет
- Confined Space Planning ChecklistДокумент3 страницыConfined Space Planning ChecklistKB100% (1)
- Treating and Preventing Ear Infections in ChildrenДокумент4 страницыTreating and Preventing Ear Infections in ChildrenbehrangОценок пока нет
- "Residential Childcare Facilities: Better Services For Namibia's Vulnerable Children" - Pact End-Of-Project ReportДокумент7 страниц"Residential Childcare Facilities: Better Services For Namibia's Vulnerable Children" - Pact End-Of-Project ReportNathan Wilkinson100% (1)
- Developmental Psychology - Socioemotional Development in Middle & Late ChildhoodДокумент56 страницDevelopmental Psychology - Socioemotional Development in Middle & Late ChildhoodAlyОценок пока нет
- Wastewater Collection Systems Comparison: William T. Hensley, International Territory Manager, Orenco Systems, IncДокумент5 страницWastewater Collection Systems Comparison: William T. Hensley, International Territory Manager, Orenco Systems, IncmeskbОценок пока нет
- Iveco F4ge PDFДокумент142 страницыIveco F4ge PDFHandy Lee67% (3)
- Mind Map Burn & BleedingДокумент2 страницыMind Map Burn & BleedingUlfia KhoirinnissaОценок пока нет
- Test Bank Contemporary Behavior Therapy - Michael-Spiegler - 6th EditionДокумент12 страницTest Bank Contemporary Behavior Therapy - Michael-Spiegler - 6th Editionlewisbacha0% (1)
- Forensic Science Project Group B5518Документ5 страницForensic Science Project Group B5518Anchit JassalОценок пока нет
- Herbal Abortifacient Drugs A ReviewДокумент6 страницHerbal Abortifacient Drugs A Reviewyogesh ushirОценок пока нет
- Plateau Pressure Ventilation MeasurementДокумент1 страницаPlateau Pressure Ventilation MeasurementImtiaz AliОценок пока нет
- Abas 3 Chapter 5Документ62 страницыAbas 3 Chapter 5GF David SalasОценок пока нет
- Surface BOP Kill SheetДокумент12 страницSurface BOP Kill Sheetzouke2002Оценок пока нет
- MAstering IATFДокумент20 страницMAstering IATFGyanesh_DBОценок пока нет
- Peaditrician All IndiaДокумент66 страницPeaditrician All IndiaGIRISH JOSHIОценок пока нет
- Aloe Vera as an Alternative Treatment for Wound HealingДокумент5 страницAloe Vera as an Alternative Treatment for Wound HealingJeffllanoОценок пока нет
- Step by Step To The Perfect PedicureДокумент6 страницStep by Step To The Perfect PedicurepinkyОценок пока нет
- A Presentation On Kit KatДокумент9 страницA Presentation On Kit KatRaju DoleyОценок пока нет
- HPAD 201 Sat Days 2 and 3Документ11 страницHPAD 201 Sat Days 2 and 3Arianne A ZamoraОценок пока нет