Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- DOCU - MedA Charting GuidelinesДокумент3 страницыDOCU - MedA Charting GuidelinesTee Wood50% (2)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- MS 2 - NCP Deep Vein ThrombosisДокумент4 страницыMS 2 - NCP Deep Vein ThrombosisDominique Excelsis J. Degamo67% (3)
- Community Health Nursing ProcessДокумент15 страницCommunity Health Nursing ProcessLheane Marley LopenaОценок пока нет
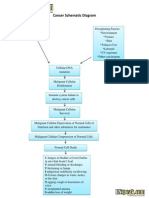
- Cancer Schematic DiagramДокумент1 страницаCancer Schematic DiagramCyrus De Asis100% (4)
- The Role of Tobacco Growing in Rural LivelihoodsДокумент28 страницThe Role of Tobacco Growing in Rural LivelihoodsIndonesia TobaccoОценок пока нет
- MauritusДокумент1 страницаMauritusIndonesia TobaccoОценок пока нет
- SpreadofVote JakartaPostДокумент1 страницаSpreadofVote JakartaPostIndonesia TobaccoОценок пока нет
- QuickCount BIДокумент1 страницаQuickCount BIIndonesia TobaccoОценок пока нет
- MalaysiaДокумент1 страницаMalaysiaIndonesia TobaccoОценок пока нет
- Master Settlement AgreementДокумент88 страницMaster Settlement AgreementIndonesia TobaccoОценок пока нет
- Community Partnership ContactsДокумент8 страницCommunity Partnership ContactsIndonesia TobaccoОценок пока нет
- The Role of Tobacco Growing in Rural LivelihoodsДокумент28 страницThe Role of Tobacco Growing in Rural LivelihoodsIndonesia TobaccoОценок пока нет
- NCDs Report Summary - WHOДокумент8 страницNCDs Report Summary - WHOIndonesia Tobacco100% (1)
- Framework Convention On Tobacco Control - FCTC EnglishДокумент42 страницыFramework Convention On Tobacco Control - FCTC EnglishIndonesia TobaccoОценок пока нет
- Rules Concerning The Ban On Smoking On European Parliament's PremiseДокумент4 страницыRules Concerning The Ban On Smoking On European Parliament's PremiseIndonesia TobaccoОценок пока нет
- LatviaДокумент1 страницаLatviaIndonesia TobaccoОценок пока нет
- Exposure To Environmental Tobacco Smoke Among South Korean AdultsДокумент33 страницыExposure To Environmental Tobacco Smoke Among South Korean AdultsIndonesia TobaccoОценок пока нет
- The Industry Menthol ReportДокумент250 страницThe Industry Menthol ReportIndonesia TobaccoОценок пока нет
- ThailandДокумент1 страницаThailandIndonesia TobaccoОценок пока нет
- SingaporeДокумент1 страницаSingaporeIndonesia TobaccoОценок пока нет
- Source: WHOДокумент2 страницыSource: WHOIndonesia TobaccoОценок пока нет
- PakistanДокумент1 страницаPakistanIndonesia TobaccoОценок пока нет
- CanadaДокумент2 страницыCanadaIndonesia TobaccoОценок пока нет
- EgyptДокумент1 страницаEgyptIndonesia TobaccoОценок пока нет
- IranДокумент1 страницаIranIndonesia TobaccoОценок пока нет
- JordanДокумент1 страницаJordanIndonesia TobaccoОценок пока нет
- IndiaДокумент1 страницаIndiaIndonesia TobaccoОценок пока нет
- BruneiДокумент1 страницаBruneiIndonesia TobaccoОценок пока нет
- AustraliaДокумент4 страницыAustraliaIndonesia TobaccoОценок пока нет
- BrazilДокумент2 страницыBrazilIndonesia TobaccoОценок пока нет
- VenezuelaДокумент2 страницыVenezuelaIndonesia TobaccoОценок пока нет
- DunhillДокумент1 страницаDunhillIndonesia TobaccoОценок пока нет
- Googling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersДокумент16 страницGoogling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersIndonesia TobaccoОценок пока нет
- DjarumДокумент4 страницыDjarumIndonesia TobaccoОценок пока нет
- Epidemiology and Outcomes of Burn Injuries at A Tertiary Burn Care Center in BangladeshДокумент7 страницEpidemiology and Outcomes of Burn Injuries at A Tertiary Burn Care Center in BangladeshE.sundara BharathiОценок пока нет
- Jurnal Maternitas Ibu HamilДокумент8 страницJurnal Maternitas Ibu HamilriswandaОценок пока нет
- Letter To Parents From Southside ISDДокумент2 страницыLetter To Parents From Southside ISDCody KingОценок пока нет
- Foundations of EpidemiologyДокумент106 страницFoundations of EpidemiologySudaysi AbdisalamОценок пока нет
- NCP OrthoДокумент7 страницNCP OrthoShewit AbrahamОценок пока нет
- Dr. Wisman's Hematology ReferenceДокумент38 страницDr. Wisman's Hematology ReferenceYpoxazОценок пока нет
- Health Risks of SmokingДокумент22 страницыHealth Risks of SmokingAhmed SakrОценок пока нет
- Surviving Sepsis Campaign Hour 1 BundleДокумент5 страницSurviving Sepsis Campaign Hour 1 BundleNadine Noelle AgraviadorОценок пока нет
- 236 297Документ8 страниц236 297Andrea KamóОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakatiarОценок пока нет
- AS Level - Infectious Diseases (CH10) Summarised NotesДокумент31 страницаAS Level - Infectious Diseases (CH10) Summarised NotesRishika Pasupulati100% (1)
- Form Annex B MDH Intan Daya 3Документ3 страницыForm Annex B MDH Intan Daya 3fajar jatmikoОценок пока нет
- Speech Hiv AidsДокумент4 страницыSpeech Hiv AidsAtika Andayani SelianОценок пока нет
- DR - REVATI - IMMUNE MEDIATED DISEASES OF OROFACIAL REGION - RevatiДокумент72 страницыDR - REVATI - IMMUNE MEDIATED DISEASES OF OROFACIAL REGION - RevatiNanik AndianiОценок пока нет
- Part 2 KROK-1Документ46 страницPart 2 KROK-1Jack frimpongОценок пока нет
- Loa Loa and Onchocerca: Parasitic Filarial Worms Causing River BlindnessДокумент28 страницLoa Loa and Onchocerca: Parasitic Filarial Worms Causing River Blindnessbindu dhanapalОценок пока нет
- Role of Automated Breast Ultrasound in Diagnostic and Early Detection 5-1Документ47 страницRole of Automated Breast Ultrasound in Diagnostic and Early Detection 5-1Dokdem AjaОценок пока нет
- Epidemiology of Inectious DiseasesДокумент23 страницыEpidemiology of Inectious DiseasesAshish ShresthaОценок пока нет
- Translate UsuДокумент8 страницTranslate UsuGhina SalsabilaОценок пока нет
- IATF Resolution No106-AДокумент5 страницIATF Resolution No106-ARappler100% (1)
- Pathophysiology of AtherosclerosisДокумент4 страницыPathophysiology of AtherosclerosisHardi AhmedОценок пока нет
- Chapoco - Course Task - NCPДокумент1 страницаChapoco - Course Task - NCPsofia yapОценок пока нет
- Babesia MicrotiДокумент9 страницBabesia MicrotiFrancene Ac-DaОценок пока нет
- 011-HSE-L203E-03 Medical Emergency Response PlanДокумент17 страниц011-HSE-L203E-03 Medical Emergency Response PlanRizky SatriawanОценок пока нет
- Amicus of ADHSДокумент35 страницAmicus of ADHScronkitenewsОценок пока нет
- 8 Bene of Ginger ShotsДокумент7 страниц8 Bene of Ginger ShotsGingkoОценок пока нет