Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Robbins Basic Pathology 9th Edition Kumar Test BankДокумент25 страницRobbins Basic Pathology 9th Edition Kumar Test BankJamesGonzalezwbpg100% (43)
- Deep Vein Thrombosis (DVT)Документ13 страницDeep Vein Thrombosis (DVT)Vijay AnandОценок пока нет
- PG Neet Obg Mcqs 90 - Malpresentation and Obstructed Labour - 1Документ15 страницPG Neet Obg Mcqs 90 - Malpresentation and Obstructed Labour - 1أ.م.د. ايناس جليل حسينОценок пока нет
- Human Diseases Case Study 19CДокумент3 страницыHuman Diseases Case Study 19Cairickann50% (2)
- Endothermal Induced ThrombosisДокумент12 страницEndothermal Induced Thrombosismarilenny santanaОценок пока нет
- Pead 3 - Abdominal Pain and VommitingДокумент22 страницыPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Guideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisДокумент18 страницGuideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisbbyesОценок пока нет
- Pead 1 - NeonatologyДокумент21 страницаPead 1 - NeonatologybbyesОценок пока нет
- Tocolytics in PretermДокумент13 страницTocolytics in PretermbbyesОценок пока нет
- Early Pregnancy ComplciationsДокумент43 страницыEarly Pregnancy ComplciationsbbyesОценок пока нет
- Training Manual 2020Документ53 страницыTraining Manual 2020bbyesОценок пока нет
- HMO Surgical PositionДокумент4 страницыHMO Surgical PositionbbyesОценок пока нет
- Substance Abuse in PregnancyДокумент151 страницаSubstance Abuse in PregnancybbyesОценок пока нет
- Prenatal ScreeningДокумент26 страницPrenatal ScreeningbbyesОценок пока нет
- C SpineДокумент44 страницыC SpinebbyesОценок пока нет
- Post Operative HypotensionДокумент7 страницPost Operative HypotensionbbyesОценок пока нет
- Weekly SDS Topics: Week 3Документ1 страницаWeekly SDS Topics: Week 3bbyesОценок пока нет
- Atrial Fibrillation Managing Acute Atrial FibrillationДокумент8 страницAtrial Fibrillation Managing Acute Atrial FibrillationbbyesОценок пока нет
- Upper GI BleedДокумент8 страницUpper GI BleedbbyesОценок пока нет
- Main Presentations of Sexually Transmitted Infections in MenДокумент3 страницыMain Presentations of Sexually Transmitted Infections in MenbbyesОценок пока нет
- ECGs - UpdatedДокумент26 страницECGs - UpdatedbbyesОценок пока нет
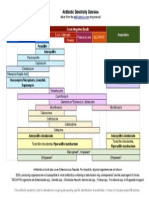
- Antibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesДокумент1 страницаAntibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesGuillermo Damian RodriguezОценок пока нет
- Colorectal Cancer: Stephen SmithДокумент33 страницыColorectal Cancer: Stephen SmithbbyesОценок пока нет
- CDR Summary - The Charlotte RuleДокумент1 страницаCDR Summary - The Charlotte RulebbyesОценок пока нет
- The Approach To Someone With The First SeizureДокумент8 страницThe Approach To Someone With The First SeizurebbyesОценок пока нет
- Simplified Wells ScoreДокумент1 страницаSimplified Wells ScorebbyesОценок пока нет
- Q1. What Is An Abscess?Документ24 страницыQ1. What Is An Abscess?bbyesОценок пока нет
- Part 1 Examination: Candidates Must Answer All Questions. Each Question Is Worth A Total of 25 MarksДокумент15 страницPart 1 Examination: Candidates Must Answer All Questions. Each Question Is Worth A Total of 25 MarksSyed Danish AliОценок пока нет
- Manual Estim Sys InstructionДокумент28 страницManual Estim Sys InstructionjhonnyОценок пока нет
- Koigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyДокумент8 страницKoigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyGATHERE KOIGIОценок пока нет
- Management of Lower Extremity Pain From Chronic Venous Insufficiency: A Comprehensive ReviewДокумент30 страницManagement of Lower Extremity Pain From Chronic Venous Insufficiency: A Comprehensive Reviewangeline chandraОценок пока нет
- Mesenteric IschemiaДокумент13 страницMesenteric IschemiaRemananОценок пока нет
- Anti-Coagulants & Fibrinolytics Feb 2019Документ50 страницAnti-Coagulants & Fibrinolytics Feb 2019Muhd NuhОценок пока нет
- Lesson 6-Cardiovascular System PDFДокумент10 страницLesson 6-Cardiovascular System PDFRichard John IslaОценок пока нет
- RCP - Post Stroke Scalp Acupuncture Research PDFДокумент64 страницыRCP - Post Stroke Scalp Acupuncture Research PDFIstiqomah Flx100% (1)
- Fragmin PT InfoДокумент5 страницFragmin PT InfoCrystal MoormanОценок пока нет
- Prometric Mock TestДокумент36 страницPrometric Mock TestDhakshina PriyaОценок пока нет
- Nursing Care of Women With Complications After BirthДокумент32 страницыNursing Care of Women With Complications After BirthHailey MooreheadОценок пока нет
- Peer Reviewed Medical Papers Submitted To Various Medical Journals, Evidencing A Multitude of Adverse Events in Covid-19 Vaccine RecipientsДокумент77 страницPeer Reviewed Medical Papers Submitted To Various Medical Journals, Evidencing A Multitude of Adverse Events in Covid-19 Vaccine RecipientsKraft DinnerОценок пока нет
- Immunology - 2022 - Chen - New Onset Autoimmune Phenomena Post COVID 19 Vaccination-1Документ17 страницImmunology - 2022 - Chen - New Onset Autoimmune Phenomena Post COVID 19 Vaccination-1Ivan StojanovicОценок пока нет
- Concept MapДокумент4 страницыConcept MapDud AccОценок пока нет
- Diagnosis of Vascular Cognitive ImpairmentДокумент17 страницDiagnosis of Vascular Cognitive ImpairmentInes Strenja LinićОценок пока нет
- Acute Lymphocytic LeukemiaДокумент8 страницAcute Lymphocytic LeukemiaWendy EscalanteОценок пока нет
- Neurology Clerkship UWORLD: Brain TumoursДокумент13 страницNeurology Clerkship UWORLD: Brain TumoursHaadi AliОценок пока нет
- Pathology of Hemodynamic Disorders 1 and 2 Practice Questions-1Документ26 страницPathology of Hemodynamic Disorders 1 and 2 Practice Questions-1JCОценок пока нет
- Medical Health Care PowerPoint TemplatesДокумент25 страницMedical Health Care PowerPoint TemplatesJeca AdornadoОценок пока нет
- Patho Common Stuff - RobbinsДокумент7 страницPatho Common Stuff - RobbinsMaf BОценок пока нет
- Common Postmortem Computed Tomography Findings Following Atraumatic Death - Differentiation Between Normal Postmortem Changes and Pathologic LesionsДокумент12 страницCommon Postmortem Computed Tomography Findings Following Atraumatic Death - Differentiation Between Normal Postmortem Changes and Pathologic LesionsFrédérique ThicotОценок пока нет
- Thesis MedicineДокумент110 страницThesis MedicineVenkatesh KorapakaОценок пока нет
- AkiДокумент20 страницAkiEnvhy AmaliaОценок пока нет
- Ready To Use Tisseel - Quick Reference GuideДокумент2 страницыReady To Use Tisseel - Quick Reference Guidebanguncitayam100% (1)