Вам также может понравиться
- Itin Online Pre Application Training 11 22 2019 2Документ90 страницItin Online Pre Application Training 11 22 2019 2Joeren GonzalesОценок пока нет
- Aircraft Fueling ManualДокумент277 страницAircraft Fueling ManualBianco Yep100% (5)
- Volvo VN, VHDДокумент104 страницыVolvo VN, VHDRegistr Registr63% (8)
- Pilot/Escort Vehicle Operators: Training ManualДокумент140 страницPilot/Escort Vehicle Operators: Training ManualD Rider CasanovaОценок пока нет
- Service Manual Volwot PDFДокумент104 страницыService Manual Volwot PDFNguyen NgocОценок пока нет
- Draft Eprmp Checklist For Expansion of Primary Hospital or Medical Facilities - RevisedДокумент15 страницDraft Eprmp Checklist For Expansion of Primary Hospital or Medical Facilities - Revisedatguintu80% (5)
- 1849 1862 Statutes at Large 601-779Документ200 страниц1849 1862 Statutes at Large 601-779ncwazzyОценок пока нет
- 101 Union of Filipro Employees Vs Vivar (Labor)Документ1 страница101 Union of Filipro Employees Vs Vivar (Labor)Kayelyn Lat100% (1)
- Complete Internal Audit Checklist (HSE)Документ59 страницComplete Internal Audit Checklist (HSE)Meer Jan89% (18)
- ECG Sample ReportДокумент9 страницECG Sample ReportJoeren GonzalesОценок пока нет
- Department of Transportation Medical Reference for ExaminersОт EverandDepartment of Transportation Medical Reference for ExaminersОценок пока нет
- Quality Control TFДокумент150 страницQuality Control TFPrabhat Kumar100% (2)
- 2018 Doh Ambulance License RequirementsДокумент31 страница2018 Doh Ambulance License RequirementsChris-Goldie Lorezo87% (31)
- DOH Ambulatory Surgical Clinic LTO at 1262015rev1Документ12 страницDOH Ambulatory Surgical Clinic LTO at 1262015rev1al gul50% (2)
- SNT-TC-1A 2020 ChangesДокумент33 страницыSNT-TC-1A 2020 ChangesShanmuga Navaneethan100% (5)
- dm2019 0056 1Документ33 страницыdm2019 0056 1DOH RO X RLEDОценок пока нет
- List Policies and ProceduresДокумент3 страницыList Policies and ProceduresJoeren GonzalesОценок пока нет
- Www.sefindia.orgДокумент372 страницыWww.sefindia.orgRahul KolateОценок пока нет
- Opito Medical Emergency Response Requirements Valid From 432016Документ20 страницOpito Medical Emergency Response Requirements Valid From 432016Joseph Soebroto100% (1)
- Case Study (Placenta Previa) This Is It!!!Документ68 страницCase Study (Placenta Previa) This Is It!!!Joeren Gonzales86% (14)
- Ao2018-0001 AMBULANCEДокумент31 страницаAo2018-0001 AMBULANCEJedith G. FloresОценок пока нет
- Ambulance Service SopДокумент27 страницAmbulance Service SopKlinik Radiologi70% (10)
- Amateur Radio Quick Study Guide: Technician Class, July 1, 2018 - June 30, 2022От EverandAmateur Radio Quick Study Guide: Technician Class, July 1, 2018 - June 30, 2022Рейтинг: 1 из 5 звезд1/5 (1)
- Ambu License Ao-2018-0001Документ39 страницAmbu License Ao-2018-0001Pdrrmo Planning100% (1)
- Measurement System AnalysisДокумент42 страницыMeasurement System Analysisazadsingh1Оценок пока нет
- Fleet Maintenance Plan Example 2-11Документ16 страницFleet Maintenance Plan Example 2-11shabkhaiz100% (1)
- Ao 2018-001Документ31 страницаAo 2018-001MedFlight Ambulance corpОценок пока нет
- Assessment Tool - Level 1 HospitalДокумент46 страницAssessment Tool - Level 1 HospitalAnne Gravador-Nepomuceno100% (1)
- Logbook TemplateДокумент3 страницыLogbook TemplateJoeren GonzalesОценок пока нет
- APP-KSMC-127 - (V4) - Crash Cart Checking & Maintenance Rev120314Документ8 страницAPP-KSMC-127 - (V4) - Crash Cart Checking & Maintenance Rev120314Kimberly Solis100% (2)
- Component Maintenance Manual With Illustrated Part ListДокумент19 страницComponent Maintenance Manual With Illustrated Part ListVeritec DocsОценок пока нет
- SampleДокумент5 страницSampleFitrah AchrianiОценок пока нет
- Renault Group Customer Specific Requirements For IATF 16949 - July 2017 - tcm183-1169110Документ10 страницRenault Group Customer Specific Requirements For IATF 16949 - July 2017 - tcm183-1169110Gonzalo MazaОценок пока нет
- The Manufacture of Sterile Pharmaceuticals and Liquid Medical Devices Using Blow-Fill-Seal Technology: Points to ConsiderОт EverandThe Manufacture of Sterile Pharmaceuticals and Liquid Medical Devices Using Blow-Fill-Seal Technology: Points to ConsiderОценок пока нет
- Assessment Tool For Licensing A Land Ambulance and Ambulance Service ProviderДокумент13 страницAssessment Tool For Licensing A Land Ambulance and Ambulance Service ProviderKaren Marjorie Nunez0% (1)
- Leak Detection and RepairДокумент8 страницLeak Detection and RepairNos GoteОценок пока нет
- Guidelines for African Swine Fever (ASF) prevention and Control in Smallholder Pig Farming in Asia: Clean Chain Approach for African Swine Fever in Smallholder SettingsОт EverandGuidelines for African Swine Fever (ASF) prevention and Control in Smallholder Pig Farming in Asia: Clean Chain Approach for African Swine Fever in Smallholder SettingsОценок пока нет
- MSA & Destructive TestДокумент4 страницыMSA & Destructive Testanon_902607157100% (1)
- Assessment Tool For Licensing A Land Ambulance and Ambulance Service ProviderДокумент14 страницAssessment Tool For Licensing A Land Ambulance and Ambulance Service ProviderMercy De GuzmanОценок пока нет
- Assessment-Tool-For-Ambulance 2018 PDFДокумент12 страницAssessment-Tool-For-Ambulance 2018 PDFDerrick ChavezОценок пока нет
- Rev2 4132015 Mfows Coa atДокумент7 страницRev2 4132015 Mfows Coa atGlenn PecoroОценок пока нет
- Ib-1-2016 NCC SpoДокумент8 страницIb-1-2016 NCC SpoPero PericОценок пока нет
- Chesar3userManual enДокумент38 страницChesar3userManual ensebicsОценок пока нет
- Idaho FC20 Reference Manual Rev 0Документ0 страницIdaho FC20 Reference Manual Rev 0Mark ReinhardtОценок пока нет
- Procedure For Complaint Handling-AOCДокумент3 страницыProcedure For Complaint Handling-AOCMohamed EzzatОценок пока нет
- User fc20 PDFДокумент34 страницыUser fc20 PDFjesus diasОценок пока нет
- U.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Документ11 страницU.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993664214458Оценок пока нет
- NuccДокумент63 страницыNuccapi-318031783Оценок пока нет
- NoticeДокумент27 страницNoticeAntonio Edgar Vargas AlcocerОценок пока нет
- MOH Circular For Private Ambulance Operators To FollowДокумент3 страницыMOH Circular For Private Ambulance Operators To FollowT33MOTEE90Оценок пока нет
- Audit Criteria - Fees (RoRo-PTB-VehiclePedestrian) (Self Made)Документ10 страницAudit Criteria - Fees (RoRo-PTB-VehiclePedestrian) (Self Made)Jocelyn NapiereОценок пока нет
- Assessment Tool - AmbulanceДокумент12 страницAssessment Tool - AmbulanceJerome Angelo LascanoОценок пока нет
- Number: Group: DateДокумент2 страницыNumber: Group: DateAfzal ImamОценок пока нет
- Medical X-Ray Application Form (7!6!2018)Документ3 страницыMedical X-Ray Application Form (7!6!2018)andrew john l.riveraОценок пока нет
- Us Fda Approval LetterДокумент5 страницUs Fda Approval LetterNAMAN KOTHARIОценок пока нет
- DOH STANDARDS (Indicators) For LEVEL 2 HOSPITALДокумент55 страницDOH STANDARDS (Indicators) For LEVEL 2 HOSPITALMOHBARMM PlanningStaffОценок пока нет
- An Acc Reference Manual and An Acc Assessment ToolДокумент37 страницAn Acc Reference Manual and An Acc Assessment Toolrachana.karki5431Оценок пока нет
- Oit 999 0008 20 00Документ4 страницыOit 999 0008 20 00Sa Be MirОценок пока нет
- GinkwaДокумент1 страницаGinkwaMai AОценок пока нет
- Nitrox Oxide - TeledyneДокумент406 страницNitrox Oxide - TeledyneAnonymous BBX2E87aHОценок пока нет
- Guidance To ASEAN CSDT - Final - 21 Oct 2010Документ31 страницаGuidance To ASEAN CSDT - Final - 21 Oct 2010bouchra8blsОценок пока нет
- Laf - Medical X-Ray FacilityДокумент3 страницыLaf - Medical X-Ray FacilityDonabel RamosОценок пока нет
- Municipality of BugueyДокумент10 страницMunicipality of BugueyJosette Mae AtanacioОценок пока нет
- U.S. Food & Drug Administration: 10903 New Hampshire Avenue Silver Spring, MD 20993Документ6 страницU.S. Food & Drug Administration: 10903 New Hampshire Avenue Silver Spring, MD 20993JebakumarОценок пока нет
- Appraisal Committee ManualДокумент17 страницAppraisal Committee ManualWorstWitch TalaОценок пока нет
- Apimf GuideДокумент10 страницApimf GuideunknowndoctorОценок пока нет
- TAC - TR - Hilux (End Out Line Marker Lamp)Документ50 страницTAC - TR - Hilux (End Out Line Marker Lamp)ankurОценок пока нет
- Aplac MR 003: (Please Type or Write Clearly in Block Letters) (Please Refer To The Notes in Appendix 1 For Guidance)Документ9 страницAplac MR 003: (Please Type or Write Clearly in Block Letters) (Please Refer To The Notes in Appendix 1 For Guidance)Rizky HarisandiОценок пока нет
- Food Control System Assessment Tool: Dimension A – Inputs and ResourcesОт EverandFood Control System Assessment Tool: Dimension A – Inputs and ResourcesОценок пока нет
- Guideline for EN 9100:2018: An Introduction to the European Aerospace and Defence StandardОт EverandGuideline for EN 9100:2018: An Introduction to the European Aerospace and Defence StandardОценок пока нет
- Nurse Form 3 Verification of Other Professional Licensure/CertificationДокумент2 страницыNurse Form 3 Verification of Other Professional Licensure/CertificationJoeren GonzalesОценок пока нет
- Exam App InstructionsДокумент22 страницыExam App InstructionsJoeren GonzalesОценок пока нет
- Patient'S Rights and Responsibilities: Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital IncДокумент8 страницPatient'S Rights and Responsibilities: Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital IncJoeren GonzalesОценок пока нет
- Hospital Formulary: Page - 0Документ11 страницHospital Formulary: Page - 0Joeren GonzalesОценок пока нет
- Kelly (Curve/medium) 10 Kelly (Curve/small) 10 Ochsner (Straight/big) 6 Ochsner (Curve/big) 6Документ1 страницаKelly (Curve/medium) 10 Kelly (Curve/small) 10 Ochsner (Straight/big) 6 Ochsner (Curve/big) 6Joeren GonzalesОценок пока нет
- Chi Square TableДокумент1 страницаChi Square TableJoeren GonzalesОценок пока нет
- Critical Values of Pearson's RДокумент1 страницаCritical Values of Pearson's RJoeren GonzalesОценок пока нет
- Nurse Deployment Project Application FormДокумент2 страницыNurse Deployment Project Application FormJoeren GonzalesОценок пока нет
- Job AnalysisДокумент10 страницJob AnalysisJoeren GonzalesОценок пока нет
- Governance of Cyber Security Research ProposalДокумент1 страницаGovernance of Cyber Security Research ProposalAleksandar MaričićОценок пока нет
- VM PDFДокумент4 страницыVM PDFTembre Rueda RaúlОценок пока нет
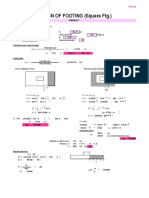
- Design of Footing (Square FTG.) : M Say, L 3.75Документ2 страницыDesign of Footing (Square FTG.) : M Say, L 3.75victoriaОценок пока нет
- Bill (Law) : Jump To Navigation Jump To SearchДокумент9 страницBill (Law) : Jump To Navigation Jump To SearchPunitОценок пока нет
- CPC Project PDFДокумент18 страницCPC Project PDFsiddharthОценок пока нет
- The Consulting Services For PreparationДокумент50 страницThe Consulting Services For PreparationJay PanitanОценок пока нет
- HDMI CABLES PERFORMANCE EVALUATION & TESTING REPORT #1 - 50FT 15M+ LENGTH CABLES v3 SMLДокумент11 страницHDMI CABLES PERFORMANCE EVALUATION & TESTING REPORT #1 - 50FT 15M+ LENGTH CABLES v3 SMLxojerax814Оценок пока нет
- Forod 2bac en s2 6 PDFДокумент4 страницыForod 2bac en s2 6 PDFwwe foreverОценок пока нет
- Khrone 5 Beam Flow Meter DatasheetДокумент16 страницKhrone 5 Beam Flow Meter DatasheetAnoop ChulliyanОценок пока нет
- E-Booklet Tacompact Board 2021Документ6 страницE-Booklet Tacompact Board 2021embenОценок пока нет
- EquisetopsidaДокумент4 страницыEquisetopsidax456456456xОценок пока нет
- Siemens Power Engineering Guide 7E 223Документ1 страницаSiemens Power Engineering Guide 7E 223mydearteacherОценок пока нет
- SS 671Документ9 страницSS 671OwОценок пока нет
- Report - Fostering The Railway Sector Through The European Green Deal PDFДокумент43 страницыReport - Fostering The Railway Sector Through The European Green Deal PDFÁdámHegyiОценок пока нет
- Hey Can I Try ThatДокумент20 страницHey Can I Try Thatapi-273078602Оценок пока нет
- Material Safety Data Sheet: Pilot IIДокумент7 страницMaterial Safety Data Sheet: Pilot IIBeyar. ShОценок пока нет
- VMC Ballscrew 32mm Horizontal Plane ReplacementДокумент11 страницVMC Ballscrew 32mm Horizontal Plane ReplacementMarlon GeronimoОценок пока нет
- BS351: Financial Reporting: Learning ObjectivesДокумент3 страницыBS351: Financial Reporting: Learning ObjectivesMajeed Ullah KhanОценок пока нет
- Call For Papers ICMIC-2016Документ1 страницаCall For Papers ICMIC-2016Zellagui EnergyОценок пока нет
- Gamesa Wind Turbine Element UpgradesДокумент1 страницаGamesa Wind Turbine Element Upgradesstanislav uzunchevОценок пока нет
- Feed Water Heater ValvesДокумент4 страницыFeed Water Heater ValvesMukesh AggarwalОценок пока нет
- Why Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingДокумент6 страницWhy Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingabhiОценок пока нет
- Public Instructions For Death CorrectionsДокумент4 страницыPublic Instructions For Death CorrectionsMukuru TechnologiesОценок пока нет
- Book Shop InventoryДокумент21 страницаBook Shop InventoryAli AnsariОценок пока нет
- X25Документ10 страницX25RajОценок пока нет