Вам также может понравиться
- Thrombosis and EmbolismДокумент43 страницыThrombosis and Embolismkanchana pvnОценок пока нет
- REport in BAcon B-CirculTORY MnintenNCEzДокумент13 страницREport in BAcon B-CirculTORY MnintenNCEzace_clemente20052266Оценок пока нет
- Classification: ArterialДокумент2 страницыClassification: ArterialKimberly DescuatanОценок пока нет
- 04 Thrombosis - Infarction.lectureДокумент81 страница04 Thrombosis - Infarction.lectureraanja2Оценок пока нет
- Is and ThrombosisДокумент5 страницIs and ThrombosisQurat KhanОценок пока нет
- Circulatory Disturbance 2Документ38 страницCirculatory Disturbance 2امينو عبدوОценок пока нет
- 02.16.1 - Thrombosis II FINAL PDFДокумент38 страниц02.16.1 - Thrombosis II FINAL PDFmaria sintaОценок пока нет
- Thrombosis: Pgi Ricky G. JalecoДокумент34 страницыThrombosis: Pgi Ricky G. JalecoRicky JalecoОценок пока нет
- Hemodynamic Disorders-Practice 36Документ39 страницHemodynamic Disorders-Practice 36Anushka SharmaОценок пока нет
- 6 Thrombosis MorphologyДокумент20 страниц6 Thrombosis MorphologySawera RaheemОценок пока нет
- Lecture 6Документ4 страницыLecture 63D2YAmvsОценок пока нет
- ThrombosisДокумент27 страницThrombosischaritykimberly3Оценок пока нет
- 2 Embolism, Infarction and ShockДокумент57 страниц2 Embolism, Infarction and ShockSuman MahmoodОценок пока нет
- Cvspa03 ThromboembolismДокумент7 страницCvspa03 ThromboembolismRobert So JrОценок пока нет
- Thrombosis: Thrombus Is Blood That Has Clotted in The Heart or A Blood VesselДокумент53 страницыThrombosis: Thrombus Is Blood That Has Clotted in The Heart or A Blood VesselhjjhОценок пока нет
- ThrombosisДокумент11 страницThrombosisNobby Onist JuniorОценок пока нет
- 6 ThrombosisДокумент27 страниц6 ThrombosisBravan AliennОценок пока нет
- Embolism and InfarctionДокумент59 страницEmbolism and InfarctionIsuri GanОценок пока нет
- Kuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockДокумент37 страницKuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockAnonymous N2PHMnTIYLОценок пока нет
- AtherosclerosisДокумент1 страницаAtherosclerosisHenky EmОценок пока нет
- Underwood: Chapter 6: Thrombosis, Embolism and InfarctionДокумент12 страницUnderwood: Chapter 6: Thrombosis, Embolism and InfarctionnyangaraОценок пока нет
- Vascular Tumors: Infantile HemangiomaДокумент4 страницыVascular Tumors: Infantile HemangiomavicenteturasОценок пока нет
- Thrombosis and Embolism: by Dr. Maha M. AbuhashimДокумент34 страницыThrombosis and Embolism: by Dr. Maha M. AbuhashimRaja EllysyaОценок пока нет
- Underwood: Chapter 6: Thrombosis, Embolism and InfarctionДокумент12 страницUnderwood: Chapter 6: Thrombosis, Embolism and InfarctionSAОценок пока нет
- 7 Embolism, Infarction & ShockДокумент57 страниц7 Embolism, Infarction & Shockجهاد مالك حاتم حسينОценок пока нет
- DVT & PeДокумент1 страницаDVT & Pea195800Оценок пока нет
- Thrombosis Is The Process of Formation of Solid Mass in Circulation From The Constituents ofДокумент11 страницThrombosis Is The Process of Formation of Solid Mass in Circulation From The Constituents ofIsak ShatikaОценок пока нет
- Emailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFДокумент38 страницEmailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFHaykal FathirrahmanОценок пока нет
- AneurysmДокумент40 страницAneurysmRichardОценок пока нет
- Case Study On Pulmonary EmbolismДокумент12 страницCase Study On Pulmonary EmbolismJobelle Acena100% (2)
- Hemodynamic DearrangementДокумент78 страницHemodynamic Dearrangementapi-19916399Оценок пока нет
- Answers: Hemodynamic ChangesДокумент8 страницAnswers: Hemodynamic ChangesUday KolheОценок пока нет
- Path-09 CARDIOДокумент18 страницPath-09 CARDIOCarlos Fernando Banegas FloresОценок пока нет
- Deep Venous ThrombosisДокумент29 страницDeep Venous Thrombosisngohonganh.hmuОценок пока нет
- 9 ThrombosisДокумент18 страниц9 ThrombosisEslam Almassri100% (1)
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismДокумент4 страницыPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- Anatomy and PhysiologyДокумент3 страницыAnatomy and PhysiologyKobe ManuelОценок пока нет
- EmbolismДокумент8 страницEmbolismBelén TapiaОценок пока нет
- Embolism & InfarctionДокумент27 страницEmbolism & InfarctionAsutosh PradhanОценок пока нет
- Pathology RCR1 CardioДокумент6 страницPathology RCR1 CardioeamcrawleyОценок пока нет
- Hemodynamic Disorders NotesДокумент12 страницHemodynamic Disorders NotesavidadarkestevilОценок пока нет
- Pulmonary Embolism: Patient EducationДокумент2 страницыPulmonary Embolism: Patient Educationyogurt100% (1)
- 5 - Aneurysms6Документ20 страниц5 - Aneurysms6Febriyant PurnomoОценок пока нет
- Myocardial InfarctionДокумент15 страницMyocardial InfarctionameerОценок пока нет
- 141 - PDFsam - Robbins & Cotran Pathologic Basis of Disease, 9eДокумент20 страниц141 - PDFsam - Robbins & Cotran Pathologic Basis of Disease, 9eRizky Angga PerdanaОценок пока нет
- Lecture 18 - ThrombosisДокумент32 страницыLecture 18 - Thrombosisapi-3703352100% (2)
- 4 CVDДокумент19 страниц4 CVDYousef WardatОценок пока нет
- Pulmonory EmbolismДокумент39 страницPulmonory EmbolismLujain M. YumenОценок пока нет
- Embolism and Infarction: Dr. Marwa Ali AbdulnabiДокумент37 страницEmbolism and Infarction: Dr. Marwa Ali Abdulnabiعلي حميد فريحОценок пока нет
- Hemodynamic Disorders, Thromoboembolism and ShockДокумент10 страницHemodynamic Disorders, Thromoboembolism and ShockMarinelle TumanguilОценок пока нет
- Circulatory Disturbance - Thombosism, Emolism, ShockДокумент16 страницCirculatory Disturbance - Thombosism, Emolism, ShockSaima ParveenОценок пока нет
- Patomorfologia Prezentacja - KopiaДокумент14 страницPatomorfologia Prezentacja - KopiaOlgaОценок пока нет
- Feline Arterial Thromboembolism - (PDF) - in EnglishДокумент7 страницFeline Arterial Thromboembolism - (PDF) - in EnglishjedicitoОценок пока нет
- Praktikum Cardiovaskular DiseaseДокумент38 страницPraktikum Cardiovaskular DiseaseJAQUELINEОценок пока нет
- AnuerysmthesisДокумент14 страницAnuerysmthesisLeahbelle ReginioОценок пока нет
- Hemodynamic Disorders - REVIEWERДокумент9 страницHemodynamic Disorders - REVIEWERDexcel concepcionОценок пока нет
- Thrombosis and EmbolismДокумент45 страницThrombosis and EmbolismJeena RajОценок пока нет
- Acute Ischemic Stroke: Etiology, Pathophysiology, Clinical Features, Diagnostics, TreatmentДокумент7 страницAcute Ischemic Stroke: Etiology, Pathophysiology, Clinical Features, Diagnostics, TreatmentAfrah AbdulОценок пока нет
- A Simple Guide to Arteriovenous Malformations, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Arteriovenous Malformations, Diagnosis, Treatment and Related ConditionsОценок пока нет
- Crs Peripheral Artery Disease - Billi Brian GeniroДокумент21 страницаCrs Peripheral Artery Disease - Billi Brian Genirofathiya nurkhalisaОценок пока нет
- MGA21324 - DefiMonitor XD - GB - JДокумент102 страницыMGA21324 - DefiMonitor XD - GB - JJulio Benancio ZuluagaОценок пока нет
- DVT, Pe, StrokeДокумент17 страницDVT, Pe, Strokezollkranzborgess50% (2)
- Guide To Cardiac Catheterization, Angioplasty, and Stent Implantation FINALДокумент4 страницыGuide To Cardiac Catheterization, Angioplasty, and Stent Implantation FINALShivani YadavОценок пока нет
- Atropine - Symptomatic BradycardiaДокумент1 страницаAtropine - Symptomatic BradycardiaSibel ErtuğrulОценок пока нет
- JURNAL Diseksi AortaДокумент3 страницыJURNAL Diseksi AortaNurhidayantiAyaMSОценок пока нет
- English For Nurses-Vital Signs and MonitoringДокумент5 страницEnglish For Nurses-Vital Signs and MonitoringSorana PaleuОценок пока нет
- ArythmiaДокумент345 страницArythmiaMuhammad ArifinОценок пока нет
- Cardiac Arrest: Signs and SymptomsДокумент7 страницCardiac Arrest: Signs and SymptomsWebster The-TechGuy LunguОценок пока нет
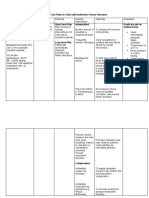
- Nursing Care Plan For Client With Ineffective Tissue PerfusionДокумент2 страницыNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayОценок пока нет
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusДокумент7 страницEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloОценок пока нет
- ANP 1105 Blood VesselsДокумент72 страницыANP 1105 Blood VesselsMathios TigerosОценок пока нет
- Adult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateДокумент1 страницаAdult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateRyggie Comelon0% (1)
- How To Make A GenogramДокумент1 страницаHow To Make A GenogramAnnaMaeGacutanMarantanОценок пока нет
- Aortic GuidelinesДокумент62 страницыAortic GuidelinesAmy Hoo Hui MayОценок пока нет
- Medical Equipment - DefibrillatorДокумент25 страницMedical Equipment - DefibrillatorLem PaneloОценок пока нет
- Body System 2º EnriqueДокумент9 страницBody System 2º EnriqueRUIZ CANO EnriqueОценок пока нет
- Heart SoundsДокумент3 страницыHeart Soundsمحمد نعيمОценок пока нет
- Penyakit Jantung Tiroid2Документ30 страницPenyakit Jantung Tiroid2Yunan ElfaОценок пока нет
- Cardiovascular Lecture Notes: AnginaДокумент23 страницыCardiovascular Lecture Notes: AnginaAnonymous iG0DCOfОценок пока нет
- CVPДокумент2 страницыCVPdrvcbОценок пока нет
- EdemaДокумент39 страницEdemaMariyah Qibtiyyah Al JufriОценок пока нет
- Cardiac VectorДокумент14 страницCardiac Vectorswastik baratОценок пока нет
- PEDIA - Acquired Heart DiseaseДокумент5 страницPEDIA - Acquired Heart DiseaseStephen Pilar PortilloОценок пока нет
- Chapter 09 Vital SignsДокумент36 страницChapter 09 Vital SignsAnnie PriscillaОценок пока нет
- 127-Article Text-817-6-10-20180329Документ4 страницы127-Article Text-817-6-10-20180329Riri Andriani MinHoОценок пока нет
- ECG Interpretation - 1 The QRS Axis The Isoelectric Lead MethodДокумент1 страницаECG Interpretation - 1 The QRS Axis The Isoelectric Lead MethodMuhammad Nurzakky100% (1)
- Ian ReportДокумент19 страницIan Reportjoyrena ochondraОценок пока нет
- Kami Export - Cardiovascular System Lecture Outline 1st PeriodДокумент16 страницKami Export - Cardiovascular System Lecture Outline 1st PeriodJada NovakОценок пока нет
- Six-Minute Walk TestДокумент2 страницыSix-Minute Walk TestExo LoveОценок пока нет