Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- BBM - 978 3 319 23458 8/1 PDFДокумент22 страницыBBM - 978 3 319 23458 8/1 PDFmedicalОценок пока нет
- JUH Residency Exam 2016Документ9 страницJUH Residency Exam 2016Nashaat H. AlshawabkehОценок пока нет
- 2017 Residancy Exam JUHДокумент8 страниц2017 Residancy Exam JUHMohammadSAL-RawashdehОценок пока нет
- 2015 Residancy Exam JUHДокумент6 страниц2015 Residancy Exam JUHMohammadSAL-RawashdehОценок пока нет
- ملخص عن حب الشبابДокумент10 страницملخص عن حب الشبابMohammadSAL-RawashdehОценок пока нет
- Sylfonylurea: Class Generic Trade Store NotesДокумент4 страницыSylfonylurea: Class Generic Trade Store NotesMohammadSAL-RawashdehОценок пока нет
- Eau 2020 PDFДокумент1 563 страницыEau 2020 PDFMirellaОценок пока нет
- Chapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterДокумент6 страницChapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterMohammadSAL-RawashdehОценок пока нет
- كتاب اسئلة جميلДокумент401 страницаكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- Tak&cha&gen&sur&uro&1st PDFДокумент321 страницаTak&cha&gen&sur&uro&1st PDFMohammadSAL-RawashdehОценок пока нет
- Gillenwater - Adult and Pediatric Urology 4th EdДокумент1 564 страницыGillenwater - Adult and Pediatric Urology 4th EdRoxana Boloaga100% (1)
- 17 - 47 HerniaДокумент68 страниц17 - 47 HerniaJoseph RichardsonОценок пока нет
- Pathophysiology of Urinary Tract PDFДокумент22 страницыPathophysiology of Urinary Tract PDFMohammadSAL-RawashdehОценок пока нет
- Eur&ass&uro&poc&gui&2020 PDFДокумент445 страницEur&ass&uro&poc&gui&2020 PDFMohammadSAL-RawashdehОценок пока нет
- Atlas 4 دائرة معارف طبية Reduced PDFДокумент316 страницAtlas 4 دائرة معارف طبية Reduced PDFMohammadSAL-RawashdehОценок пока нет
- (Mebooksfree Net) Oxf&tex&uro&sur&1stДокумент1 201 страница(Mebooksfree Net) Oxf&tex&uro&sur&1stMohammadSAL-Rawashdeh100% (2)
- (Mebooksfree - Net) Com&rev&uro&2018 OptimizedДокумент851 страница(Mebooksfree - Net) Com&rev&uro&2018 OptimizedMohammadSAL-RawashdehОценок пока нет
- Urology Sample MCQ Exam eДокумент5 страницUrology Sample MCQ Exam eMohammadSAL-RawashdehОценок пока нет
- كتاب اسئلة جميلДокумент401 страницаكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- (Mebooksfree Net) Hin&atl&uro&sur&4thДокумент967 страниц(Mebooksfree Net) Hin&atl&uro&sur&4thMohammadSAL-Rawashdeh100% (12)
- أدوية الطوارىءДокумент162 страницыأدوية الطوارىءManar22Оценок пока нет
- Shenimt e Mia Personale Per DDXДокумент281 страницаShenimt e Mia Personale Per DDXJeronim H'gharОценок пока нет
- Shenimt e Mia Personale Per DDXДокумент281 страницаShenimt e Mia Personale Per DDXJeronim H'gharОценок пока нет
- (Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndДокумент1 235 страниц(Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndMohammadSAL-Rawashdeh100% (1)
- 6 - 7 - 8 Peritoneum, Pancreas, AppendixДокумент134 страницы6 - 7 - 8 Peritoneum, Pancreas, AppendixMohammadSAL-RawashdehОценок пока нет
- Sabers HandbookДокумент35 страницSabers HandbookMohammadSAL-Rawashdeh100% (1)
- Oral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityДокумент38 страницOral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityMohammadSAL-RawashdehОценок пока нет
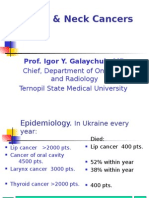
- Head & Neck Cancers: Prof. Igor Y. Galaychuk, MDДокумент43 страницыHead & Neck Cancers: Prof. Igor Y. Galaychuk, MDMohammadSAL-RawashdehОценок пока нет
- Epidemiology of Cancer. Methods of Diagnosis and TreatmentДокумент70 страницEpidemiology of Cancer. Methods of Diagnosis and TreatmentMohammadSAL-RawashdehОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Real Estate (Regulation and Development) Act 2016 (RERA) CompliancesДокумент15 страницReal Estate (Regulation and Development) Act 2016 (RERA) CompliancesM S PrasadОценок пока нет
- Defence QuestionnaireДокумент2 страницыDefence QuestionnaireSumitt SinghОценок пока нет
- Multidimensional Scaling Groenen Velden 2004 PDFДокумент14 страницMultidimensional Scaling Groenen Velden 2004 PDFjoséОценок пока нет
- New Python Basics AssignmentДокумент5 страницNew Python Basics AssignmentRAHUL SONI0% (1)
- Cs09 404 Programming Paradigm (Module 1 Notes)Документ24 страницыCs09 404 Programming Paradigm (Module 1 Notes)Rohith BhaskaranОценок пока нет
- MKT STGДокумент106 страницMKT STGAmeya Singh RajputОценок пока нет
- MBF100 Subject OutlineДокумент2 страницыMBF100 Subject OutlineMARUTI JEWELSОценок пока нет
- English Literature Coursework Aqa GcseДокумент6 страницEnglish Literature Coursework Aqa Gcsef5d17e05100% (2)
- 11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004Документ7 страниц11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004afzal taiОценок пока нет
- Far 2 Quiz 03212024Документ6 страницFar 2 Quiz 03212024red118831Оценок пока нет
- AppendixA LaplaceДокумент12 страницAppendixA LaplaceSunny SunОценок пока нет
- Cuerpos Extraños Origen FDAДокумент30 страницCuerpos Extraños Origen FDALuis GallegosОценок пока нет
- Opening The Third EyeДокумент13 страницOpening The Third EyekakamacgregorОценок пока нет
- Sci5 q3 Module3 NoanswerkeyДокумент22 страницыSci5 q3 Module3 NoanswerkeyRebishara CapobresОценок пока нет
- PDF RR Grade Sep ProjectsДокумент46 страницPDF RR Grade Sep ProjectsjunqiangdongОценок пока нет
- Lesson Plan Outline - Rebounding - Perez - JoseДокумент7 страницLesson Plan Outline - Rebounding - Perez - JoseJose PerezОценок пока нет
- Applied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1Документ36 страницApplied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1wesleyvasquezmeoapcjtrb100% (25)
- E-Cat35xt014 Xtro PhantomsДокумент32 страницыE-Cat35xt014 Xtro PhantomsKari Wilfong100% (5)
- NS1 UserManual EN V1.2Документ31 страницаNS1 UserManual EN V1.2T5 TecnologiaОценок пока нет
- InfltiДокумент13 страницInfltiLEKH021Оценок пока нет
- Statistics 2Документ121 страницаStatistics 2Ravi KОценок пока нет
- Practice Problems For Modulus and Logarithm Section-I: FiitjeeДокумент8 страницPractice Problems For Modulus and Logarithm Section-I: FiitjeePratham SharmaОценок пока нет
- Denso - History PDFДокумент5 страницDenso - History PDFVenkateswaran KrishnamurthyОценок пока нет
- Electric Vehicle Charging Station BplanДокумент19 страницElectric Vehicle Charging Station BplanAjithОценок пока нет
- Final Sent Technical Specification 14.03.2019Документ16 страницFinal Sent Technical Specification 14.03.2019harishОценок пока нет
- Antonov 225 - The Largest - Airliner in The WorldДокумент63 страницыAntonov 225 - The Largest - Airliner in The WorldFridayFunStuffОценок пока нет
- What Is The Effective Method For Dissolution of HDPE and LDPE - PDFДокумент12 страницWhat Is The Effective Method For Dissolution of HDPE and LDPE - PDFAliОценок пока нет
- Syllabus Math 305Документ4 страницыSyllabus Math 305Nataly SusanaОценок пока нет
- Understand Fox Behaviour - Discover WildlifeДокумент1 страницаUnderstand Fox Behaviour - Discover WildlifeChris V.Оценок пока нет