Вам также может понравиться
- Lower Extremity Arterial Protocol 14 PDFДокумент2 страницыLower Extremity Arterial Protocol 14 PDFapi-390240132Оценок пока нет
- Upper Extremity Arterial Protocol 14Документ3 страницыUpper Extremity Arterial Protocol 14api-349402240Оценок пока нет
- Upper Extremity Venous Protocol 14Документ2 страницыUpper Extremity Venous Protocol 14api-349402240Оценок пока нет
- Lower Extremity Venous Incompetence Protcol 14Документ5 страницLower Extremity Venous Incompetence Protcol 14api-349402240Оценок пока нет
- Renal Doppler Protocol 14 1Документ4 страницыRenal Doppler Protocol 14 1api-349402240100% (1)
- Mesenteric Doppler Protocol 14Документ2 страницыMesenteric Doppler Protocol 14api-349402240Оценок пока нет
- Lower Extremity Arterial Protocol 14 1Документ2 страницыLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- 93306Документ64 страницы93306jamesgailОценок пока нет
- Principlesofdopplerultrasound 130514165605 Phpapp02Документ92 страницыPrinciplesofdopplerultrasound 130514165605 Phpapp02csngiu100% (2)
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyДокумент23 страницыStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethОценок пока нет
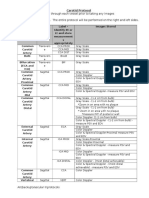
- Carotid Protocol 14 1Документ4 страницыCarotid Protocol 14 1api-349402240Оценок пока нет
- Doppler Ultrasound of The KidneysДокумент23 страницыDoppler Ultrasound of The KidneysivoklarinОценок пока нет
- Carotid Protocol 14 PDFДокумент3 страницыCarotid Protocol 14 PDFapi-390240132Оценок пока нет
- Basic of Doppler UltrasoundДокумент25 страницBasic of Doppler Ultrasoundpepsimax85Оценок пока нет
- Scrotum Protocol 14Документ2 страницыScrotum Protocol 14api-349402240Оценок пока нет
- Fetal Echocardiogram ProtocolДокумент4 страницыFetal Echocardiogram Protocolapi-349402240Оценок пока нет
- Ob Biophysical Profile Protocol r14 PDFДокумент3 страницыOb Biophysical Profile Protocol r14 PDFapi-390240132Оценок пока нет
- Lower Extremity Venous Protocol 14Документ3 страницыLower Extremity Venous Protocol 14api-276847924Оценок пока нет
- Appendix Protocol 14 1Документ2 страницыAppendix Protocol 14 1api-349402240Оценок пока нет
- 9 Muscle Teaching Slides PDFДокумент91 страница9 Muscle Teaching Slides PDFhosam jaradatОценок пока нет
- Abdominal US in Hepatobiliary DiseasesДокумент76 страницAbdominal US in Hepatobiliary DiseasesSyafari D. MangopoОценок пока нет
- Liver Protocol 14 1Документ5 страницLiver Protocol 14 1api-349402240Оценок пока нет
- Color and Power DopplerДокумент114 страницColor and Power DopplerThuraiya Al MasoudiОценок пока нет
- Abdomen Protocol 14 PDFДокумент6 страницAbdomen Protocol 14 PDFapi-390240132Оценок пока нет
- LiverultrasoundДокумент62 страницыLiverultrasoundiuliia94Оценок пока нет
- Doppler Echocardiography: Dr.S.R.Sruthi Meenaxshi MBBS, MD, PDFДокумент38 страницDoppler Echocardiography: Dr.S.R.Sruthi Meenaxshi MBBS, MD, PDFsruthimeena6891Оценок пока нет
- Policies and Statements: Peripheral Arterial UltrasoundДокумент5 страницPolicies and Statements: Peripheral Arterial UltrasoundJing CruzОценок пока нет
- 14 Clauss Pediatric Echocardiography PDFДокумент159 страниц14 Clauss Pediatric Echocardiography PDFSergiu NiculitaОценок пока нет
- Ultrasound: Made By: Conny LeoДокумент15 страницUltrasound: Made By: Conny LeoChristabelle ConnyОценок пока нет
- D5 PolicyДокумент5 страницD5 PolicyDenis PogoreviciОценок пока нет
- Pediatric Spine 14Документ2 страницыPediatric Spine 14api-349402240Оценок пока нет
- Us Abdominal AortaДокумент16 страницUs Abdominal AortaRomaОценок пока нет
- Kuliah Blok GI Tract - USG Abd - September 2010Документ65 страницKuliah Blok GI Tract - USG Abd - September 2010Natallia BatuwaelОценок пока нет
- Ultrasonography Assessment of Lower Limb VeinsДокумент49 страницUltrasonography Assessment of Lower Limb VeinsPutra AchmadОценок пока нет
- DR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging BsmmuДокумент46 страницDR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging Bsmmudr_shamimr100% (1)
- Hepatoportal DopplerДокумент15 страницHepatoportal DopplerRaj Koticha100% (1)
- Vascular Disorders StudentsДокумент70 страницVascular Disorders StudentsedwinОценок пока нет
- 1001130 - 急診基礎超音波 (CV+Chest+MSK) @羅東博愛Документ78 страниц1001130 - 急診基礎超音波 (CV+Chest+MSK) @羅東博愛juice119Оценок пока нет
- Chapter 18Документ17 страницChapter 18George LeahuОценок пока нет
- Us Vasos RetroperitonealesДокумент101 страницаUs Vasos RetroperitonealesLourdes MarcosОценок пока нет
- Ultrasound of Srotal Emergency in PediatricДокумент53 страницыUltrasound of Srotal Emergency in PediatricIsti Iryan PriantiОценок пока нет
- Apr 28 Ultrasound Chawla PDFДокумент85 страницApr 28 Ultrasound Chawla PDFAna-Maria PopaОценок пока нет
- Small Parts USДокумент58 страницSmall Parts USWaqas AliОценок пока нет
- Allen Test Protocol 14 1Документ2 страницыAllen Test Protocol 14 1api-349402240Оценок пока нет
- Normal Reference Values: DR Ayush GoelДокумент2 страницыNormal Reference Values: DR Ayush GoelNic WGTОценок пока нет
- Diastolic DysfunctionДокумент6 страницDiastolic DysfunctionMarina SecureanuОценок пока нет
- Abdominal UtzДокумент13 страницAbdominal UtzRodel AgapitoОценок пока нет
- Usg Blok 17Документ104 страницыUsg Blok 17iqiqiqiqiqОценок пока нет
- Gynecoloical Ultrasound Doppler AssessmentДокумент17 страницGynecoloical Ultrasound Doppler AssessmentKinzaОценок пока нет
- Coursebook-Echoscopy ch30Документ23 страницыCoursebook-Echoscopy ch30Сергей СадовниковОценок пока нет
- ISUOG Basic Training: Writing The Gynecological Ultrasound ReportДокумент29 страницISUOG Basic Training: Writing The Gynecological Ultrasound ReportsandrogvaladzeОценок пока нет
- Normal Variant in Abdominal UltrasounДокумент20 страницNormal Variant in Abdominal Ultrasounshanks spearsonОценок пока нет
- Chapter 33Документ14 страницChapter 33Haba HenrikОценок пока нет
- 990617 EUS教學 (12) 急診超音波在兒科急症之應用Документ67 страниц990617 EUS教學 (12) 急診超音波在兒科急症之應用juice119100% (1)
- Practice Guidlines For Performance First Trimester USДокумент95 страницPractice Guidlines For Performance First Trimester USOxy GenОценок пока нет
- Doppler US and GrowthДокумент43 страницыDoppler US and GrowthAulia rahmawatiОценок пока нет
- Lower Extremity Venous Protocol 14Документ3 страницыLower Extremity Venous Protocol 14api-349474075Оценок пока нет
- Renal Doppler Protocol 14 PDFДокумент3 страницыRenal Doppler Protocol 14 PDFapi-390240132Оценок пока нет
- CMR GuidecongenitasD 2014Документ105 страницCMR GuidecongenitasD 2014karen mendoza rodriguezОценок пока нет
- Penile UltrasoundДокумент20 страницPenile UltrasoundVincent LyncottОценок пока нет
- Case Report For Case Presentations Short Rib Polydactyly SyndromeДокумент8 страницCase Report For Case Presentations Short Rib Polydactyly Syndromeapi-390240132Оценок пока нет
- Case Presentation Powerpoint FinalДокумент13 страницCase Presentation Powerpoint Finalapi-390240132Оценок пока нет
- Stormy Laxton Hypertrophic Pyloric Stenosis Research Paper Summer 2017Документ9 страницStormy Laxton Hypertrophic Pyloric Stenosis Research Paper Summer 2017api-390240132Оценок пока нет
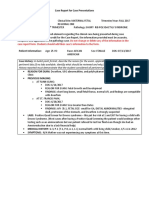
- Case Report For Case Presentations 2Документ3 страницыCase Report For Case Presentations 2api-390240132Оценок пока нет
- Stormy Laxton Case Presentation Summer 2017summer 2017Документ12 страницStormy Laxton Case Presentation Summer 2017summer 2017api-390240132Оценок пока нет
- Case Presentation - Thanatophoric DysplasiaДокумент20 страницCase Presentation - Thanatophoric Dysplasiaapi-390240132Оценок пока нет
- Scrotum Protocol 14Документ2 страницыScrotum Protocol 14api-349402240Оценок пока нет
- Lower Extremity Venous Protocol 14Документ3 страницыLower Extremity Venous Protocol 14api-349474075Оценок пока нет
- Ob First Trimester Protocol r15 PDFДокумент4 страницыOb First Trimester Protocol r15 PDFapi-390240132Оценок пока нет
- Breast Protocol 14 PDFДокумент3 страницыBreast Protocol 14 PDFapi-390240132Оценок пока нет
- Thoracic Outlet Syndrome Protocol 14 PDFДокумент1 страницаThoracic Outlet Syndrome Protocol 14 PDFapi-390240132Оценок пока нет
- Renal Doppler Protocol 14 PDFДокумент3 страницыRenal Doppler Protocol 14 PDFapi-390240132Оценок пока нет
- Upper Extremity Venous Protocol 14 PDFДокумент2 страницыUpper Extremity Venous Protocol 14 PDFapi-390240132Оценок пока нет
- Adult Echocardiography Protocol 14 PDFДокумент9 страницAdult Echocardiography Protocol 14 PDFapi-390240132Оценок пока нет
- Mesenteric Doppler Protocol 14 PDFДокумент2 страницыMesenteric Doppler Protocol 14 PDFapi-390240132Оценок пока нет
- Lower Extremity Venous Incompetence Protcol 14 PDFДокумент3 страницыLower Extremity Venous Incompetence Protcol 14 PDFapi-390240132Оценок пока нет
- Allen Test Protocol 14 1Документ2 страницыAllen Test Protocol 14 1api-349402240Оценок пока нет
- Hepatic Doppler Protocol 14 PDFДокумент3 страницыHepatic Doppler Protocol 14 PDFapi-390240132Оценок пока нет
- 2nd Trimester Protocol r14 PDFДокумент8 страниц2nd Trimester Protocol r14 PDFapi-390240132Оценок пока нет
- Pelvis Protocol r14 PDFДокумент2 страницыPelvis Protocol r14 PDFapi-390240132Оценок пока нет
- Carotid Protocol 14 PDFДокумент3 страницыCarotid Protocol 14 PDFapi-390240132Оценок пока нет
- Ob Biophysical Profile Protocol r14 PDFДокумент3 страницыOb Biophysical Profile Protocol r14 PDFapi-390240132Оценок пока нет
- Neonatal Head Protocol 14 PDFДокумент5 страницNeonatal Head Protocol 14 PDFapi-390240132Оценок пока нет
- Urinary Protocol 14 PDFДокумент3 страницыUrinary Protocol 14 PDFapi-390240132Оценок пока нет
- Pyloric Stenosis 14Документ3 страницыPyloric Stenosis 14api-349402240Оценок пока нет
- Pediatric Spine 14 PDFДокумент2 страницыPediatric Spine 14 PDFapi-390240132Оценок пока нет
- Pediatric Hip Protocol 14 PDFДокумент2 страницыPediatric Hip Protocol 14 PDFapi-390240132Оценок пока нет
- Thyroid Protocol 14 PDFДокумент2 страницыThyroid Protocol 14 PDFapi-390240132Оценок пока нет
- Smart City Scheme GuidelinesДокумент48 страницSmart City Scheme GuidelinesKarishma Juttun100% (1)
- Nursing Practice Skills: Adult Intensive Care Unit PatientsДокумент10 страницNursing Practice Skills: Adult Intensive Care Unit PatientsMona Doria67% (3)
- Grade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFДокумент6 страницGrade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFmafeh caranogОценок пока нет
- 10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtДокумент145 страниц10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtVuong DiepОценок пока нет
- EPTT5100 - Pressure - Temperature Sensor - 1308 - GДокумент2 страницыEPTT5100 - Pressure - Temperature Sensor - 1308 - GHendry Putra RahadiОценок пока нет
- Unit-3: Grid FrameworkДокумент44 страницыUnit-3: Grid FrameworkMUKESH KUMAR P 2019-2023 CSEОценок пока нет
- Manual CaladoraДокумент32 страницыManual CaladoraMiguel Angel Vega TrejoОценок пока нет
- Peethas ListДокумент1 страницаPeethas ListChetan PrajapatiОценок пока нет
- IKEA - Huntsman Positive List - 27 May 2016 - EN - FINAL - v1Документ30 страницIKEA - Huntsman Positive List - 27 May 2016 - EN - FINAL - v1Flávia DutraОценок пока нет
- Board ManualДокумент190 страницBoard ManualkmalОценок пока нет
- Basic Pancakes Recipe - Martha StewartДокумент37 страницBasic Pancakes Recipe - Martha Stewartkrishna kumarОценок пока нет
- CatalogДокумент52 страницыCatalogtalabiraОценок пока нет
- Gulika in Vedic AstrologyДокумент8 страницGulika in Vedic AstrologyCatchdgreen100% (1)
- Chapter-01 Introduction: Sonadanga Residential Area (1st Phase)Документ17 страницChapter-01 Introduction: Sonadanga Residential Area (1st Phase)MAFRID HAYDARОценок пока нет
- Proposed Bedroom Enhancement: Jenel C. Tangonan Archi 1A (Stem) Architectural Design Plate No.1Документ1 страницаProposed Bedroom Enhancement: Jenel C. Tangonan Archi 1A (Stem) Architectural Design Plate No.1Jehan TangonanОценок пока нет
- The Foods of Italy BookДокумент92 страницыThe Foods of Italy BookmanupopОценок пока нет
- At Your Service: Affordable LandscapingДокумент1 страницаAt Your Service: Affordable LandscapingDamaris HigginsОценок пока нет
- Video Wall, Digital Signage & C'Type Serial NumberДокумент8 страницVideo Wall, Digital Signage & C'Type Serial NumberAbhijit BarmanОценок пока нет
- Who Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byДокумент6 страницWho Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byJun Dl CrzОценок пока нет
- MECH0018.1 Assignment 2 QP Fall 2021Документ17 страницMECH0018.1 Assignment 2 QP Fall 2021saleem razaОценок пока нет
- Review of Henry Vyverberg, Historical Pessimism in The French EnlightenmentДокумент4 страницыReview of Henry Vyverberg, Historical Pessimism in The French EnlightenmentRalph EllectualОценок пока нет
- First Periodical Exam Math 8Документ2 страницыFirst Periodical Exam Math 8Joanne88% (8)
- Iso TR 16922 2013 (E)Документ18 страницIso TR 16922 2013 (E)Freddy Santiago Cabarcas LandinezОценок пока нет
- Vivo X5Pro Smartphone Specifications: Brand and ModelДокумент4 страницыVivo X5Pro Smartphone Specifications: Brand and ModelEric AndriantoОценок пока нет
- Mechanical Reasoning - Test 2: 40 QuestionsДокумент14 страницMechanical Reasoning - Test 2: 40 Questionskyloz60% (5)
- Higher Unit 11 Topic Test: NameДокумент17 страницHigher Unit 11 Topic Test: NamesadiyaОценок пока нет
- ABS Rules For Cable SizingДокумент2 страницыABS Rules For Cable SizingMohammed JassimОценок пока нет
- YES-O Action-Plan - 2022-2023Документ2 страницыYES-O Action-Plan - 2022-2023carmina duldulao100% (6)
- 9) Expt No - 9 (Halleffect)Документ16 страниц9) Expt No - 9 (Halleffect)Pollack Prittam ChoudhuryОценок пока нет
- Part PabrikДокумент2 страницыPart PabrikNaldy NaldyОценок пока нет