Вам также может понравиться
- Countdown 2030: Tracking Progress Towards Universal Coverage For Women's, Children's and Adolescents' HealthДокумент102 страницыCountdown 2030: Tracking Progress Towards Universal Coverage For Women's, Children's and Adolescents' Healthmaxicap73Оценок пока нет
- Newborn Essential Care PDFДокумент54 страницыNewborn Essential Care PDFMARK LENAND ESPIRITU100% (1)
- Breastfeeding in The Philippines, A Critical Review 2013Документ38 страницBreastfeeding in The Philippines, A Critical Review 2013melabernardinoОценок пока нет
- Countdown 2030: Tracking Progress Towards Universal Coverage For Women's, Children's and Adolescents' HealthДокумент102 страницыCountdown 2030: Tracking Progress Towards Universal Coverage For Women's, Children's and Adolescents' Healthmaxicap73Оценок пока нет
- Global BF Scorecard 2017Документ7 страницGlobal BF Scorecard 2017sofiabloemОценок пока нет
- Unicef Guidelines For Disability Situational AnaylsisДокумент20 страницUnicef Guidelines For Disability Situational Anaylsismaxicap73Оценок пока нет
- BF PDFДокумент85 страницBF PDFGemmith GosanesОценок пока нет
- DOH Phil Drug Price Ref Index 2013Документ23 страницыDOH Phil Drug Price Ref Index 2013maxicap73Оценок пока нет
- Joint Memorandum Circular of DOH and DILG On IP SDNДокумент3 страницыJoint Memorandum Circular of DOH and DILG On IP SDNmaxicap73Оценок пока нет
- Reading Food Label - Dec 9 2011Документ4 страницыReading Food Label - Dec 9 2011maxicap73Оценок пока нет
- DOH AO 2010 0014 Administration of Life-Saving Drugs and Medicine by Midwives-1Документ6 страницDOH AO 2010 0014 Administration of Life-Saving Drugs and Medicine by Midwives-1maxicap7367% (6)
- Einc Newborn Mar 2011Документ70 страницEinc Newborn Mar 2011maxicap73100% (2)
- EINC Bulletin VOL 3Документ8 страницEINC Bulletin VOL 3maxicap73Оценок пока нет
- ROM Exercises From Aurora Health CareДокумент3 страницыROM Exercises From Aurora Health Caremaxicap73100% (1)
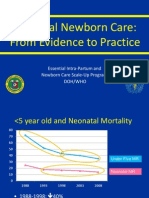
- Essential Intrapartum and Newborn Care (EINC) Bulletin 1Документ10 страницEssential Intrapartum and Newborn Care (EINC) Bulletin 1maxicap7386% (7)
- Essential Intrapartum and Newborn Care (EINC) Bulletin 1Документ10 страницEssential Intrapartum and Newborn Care (EINC) Bulletin 1maxicap7386% (7)
- Essential Intrapartum and Newborn Care (EINC) Bulletin 1Документ10 страницEssential Intrapartum and Newborn Care (EINC) Bulletin 1maxicap7386% (7)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- SEL in The Music ClassroomДокумент57 страницSEL in The Music ClassroomBabydoll MarieОценок пока нет
- IHRM And: MulticulturalismДокумент18 страницIHRM And: MulticulturalismAneeka MelwaniОценок пока нет
- Entrepreneurship Quarter1 Activity SheetsДокумент6 страницEntrepreneurship Quarter1 Activity SheetsJolly Roy BersalunaОценок пока нет
- A Presentation By:-Anuj Sachdev Gomem Gangkak Rzayak Oberoi Sanil Yadav Vaibhav PandeyДокумент11 страницA Presentation By:-Anuj Sachdev Gomem Gangkak Rzayak Oberoi Sanil Yadav Vaibhav PandeySanil YadavОценок пока нет
- TR-Pharmacy Services NC IIIДокумент136 страницTR-Pharmacy Services NC IIIAre Pee Etc100% (2)
- Erect & Dismantle of ScaffoldДокумент15 страницErect & Dismantle of Scaffoldmohammad Qutubuddin100% (2)
- F103-12-QMS-2015 ISO 9001 2015 Checklist GuidanceДокумент20 страницF103-12-QMS-2015 ISO 9001 2015 Checklist GuidanceZyrus OyongОценок пока нет
- Timoteyos Yonas HaileДокумент104 страницыTimoteyos Yonas Hailemamaru bantieОценок пока нет
- Effectiveness of Human Resource Management Practices To The Employee Productivity As Percieved by Selected Employee of Xyz CompanyДокумент74 страницыEffectiveness of Human Resource Management Practices To The Employee Productivity As Percieved by Selected Employee of Xyz CompanyAndrea Tagangin100% (1)
- Impact of Job Satisfaction On Employees Retention TV PDFДокумент48 страницImpact of Job Satisfaction On Employees Retention TV PDFAli HassanОценок пока нет
- 2.2. CIA Part One Revised Syllabus: Foundations of Internal Auditing (15%)Документ3 страницы2.2. CIA Part One Revised Syllabus: Foundations of Internal Auditing (15%)girirajОценок пока нет
- CBC TEMPLATE - Domestic Work NC IIДокумент23 страницыCBC TEMPLATE - Domestic Work NC IIemely ba-arde92% (12)
- "If Only HP Kne W What HP Knows - . .": About The AuthorДокумент6 страниц"If Only HP Kne W What HP Knows - . .": About The AuthorHevi Plasencia DíazОценок пока нет
- Srs Job DescriptionДокумент4 страницыSrs Job DescriptionMary Yole Apple DeclaroОценок пока нет
- Competency Based Interview GuideДокумент2 страницыCompetency Based Interview GuideellyciousОценок пока нет
- CBLM OhsДокумент103 страницыCBLM OhsJel Gaoiran Tacadena80% (25)
- Strategic Staffing SlidesДокумент245 страницStrategic Staffing Slidesbond485100% (8)
- Diploma Business Administration Course Outline v1-11Документ2 страницыDiploma Business Administration Course Outline v1-11Emmanuel DollarОценок пока нет
- Brochure SBL PDFДокумент8 страницBrochure SBL PDFXronia YiorgosОценок пока нет
- The Four Pillars of EducationДокумент21 страницаThe Four Pillars of Educationsyahirah mahatОценок пока нет
- Mia by Law Fundamental-ObjectivityДокумент5 страницMia by Law Fundamental-ObjectivityFatinah Husna100% (1)
- Quality in Classroom TransactionДокумент3 страницыQuality in Classroom TransactionrajmohapatraОценок пока нет
- TR - Forging NC IIIДокумент55 страницTR - Forging NC IIImerlita rivadeneraОценок пока нет
- MM5009 Strategic Decision Making and NegotiationДокумент11 страницMM5009 Strategic Decision Making and NegotiationAnanda KurniawanОценок пока нет
- Performance Management Chapter 2 ReviewДокумент5 страницPerformance Management Chapter 2 ReviewEmily VaughnОценок пока нет
- HRM in McdonaldsДокумент19 страницHRM in McdonaldsAimen Chauhdary100% (6)
- CS Plan Prepare and Display A Buffet ServiceДокумент10 страницCS Plan Prepare and Display A Buffet ServiceJarot SyamsurizalОценок пока нет
- 2017-2018 SUM Manual PDFДокумент79 страниц2017-2018 SUM Manual PDFTasheenaОценок пока нет
- Dev Plan Job Aid PDFДокумент2 страницыDev Plan Job Aid PDFMarvinОценок пока нет
- Lesson 1 PPT in MILДокумент20 страницLesson 1 PPT in MILCharlene Ann Briones100% (6)