Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Baking Soda A Cure For HumanityДокумент6 страницBaking Soda A Cure For Humanitysheriff77080% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Petroleum As A Cancer CureДокумент4 страницыPetroleum As A Cancer Curedaurel100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Nclex PointersДокумент4 страницыNclex PointersCarl Michael de Guzman75% (12)
- Activity 3.1.2 Rapid Pathogen IdentificationДокумент8 страницActivity 3.1.2 Rapid Pathogen Identificationsahsdjkh7Оценок пока нет
- PhoenixДокумент3 страницыPhoenixvicenteturas100% (1)
- EPN Book 2Документ40 страницEPN Book 2Budhi Priyanto DitaraОценок пока нет
- Homeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Документ21 страницаHomeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Yuldash100% (2)
- Medical BooksДокумент20 страницMedical Booksapi-385347264% (14)
- Organophosphate Poisoning - WikiДокумент31 страницаOrganophosphate Poisoning - WikiLIDIYA MOL P VОценок пока нет
- 3rd Yr TURASДокумент1 страница3rd Yr TURASvicenteturasОценок пока нет
- 3rd Yr TURASДокумент1 страница3rd Yr TURASvicenteturasОценок пока нет
- Saint Louis University: School of NursingДокумент1 страницаSaint Louis University: School of NursingvicenteturasОценок пока нет
- Saint Louis University: School of Nursing Family Nursing Assessment ToolДокумент2 страницыSaint Louis University: School of Nursing Family Nursing Assessment ToolvicenteturasОценок пока нет
- Saint Louis University: School of NursingДокумент5 страницSaint Louis University: School of NursingvicenteturasОценок пока нет
- 3rd Yr TURASДокумент1 страница3rd Yr TURASvicenteturasОценок пока нет
- 3rd Yr TURASДокумент1 страница3rd Yr TURASvicenteturasОценок пока нет
- Portfolio Reflective WritingДокумент8 страницPortfolio Reflective WritingvicenteturasОценок пока нет
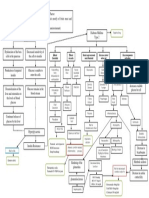
- Lack of Insulin Decreases Available Glucose For CellДокумент1 страницаLack of Insulin Decreases Available Glucose For CellvicenteturasОценок пока нет
- PricingДокумент3 страницыPricingvicenteturasОценок пока нет
- JVJV NCP Risk For Fluid Volume DeficitДокумент2 страницыJVJV NCP Risk For Fluid Volume DeficitvicenteturasОценок пока нет
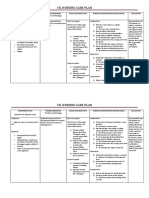
- Vii. Nursing Care PlanДокумент4 страницыVii. Nursing Care PlanvicenteturasОценок пока нет
- 3d. Family Nursing Assessment Tool Pp3 7 B 1Документ5 страниц3d. Family Nursing Assessment Tool Pp3 7 B 1vicenteturasОценок пока нет
- Saint Louis University 1Документ6 страницSaint Louis University 1vicenteturasОценок пока нет
- 3d. Family Nursing Assessment Tool Pp1 2 BДокумент2 страницы3d. Family Nursing Assessment Tool Pp1 2 BvicenteturasОценок пока нет
- Vascular Tumors: Infantile HemangiomaДокумент4 страницыVascular Tumors: Infantile HemangiomavicenteturasОценок пока нет
- 3d. Family Nursing Assessment Tool pp1 2 BДокумент2 страницы3d. Family Nursing Assessment Tool pp1 2 BvicenteturasОценок пока нет
- LumpectomyДокумент4 страницыLumpectomyvicenteturasОценок пока нет
- Blade and Blade HolderДокумент5 страницBlade and Blade HoldervicenteturasОценок пока нет
- BY:Mabatas, Mel-hanie:Daoal, Maine Celine:Turas, Vicente IIIДокумент2 страницыBY:Mabatas, Mel-hanie:Daoal, Maine Celine:Turas, Vicente IIIvicenteturasОценок пока нет
- Basal Cell Carcinoma With Lymph Node Metastasis A Case Report and Review of LiteratureДокумент5 страницBasal Cell Carcinoma With Lymph Node Metastasis A Case Report and Review of LiteratureIJAR JOURNALОценок пока нет
- Health Implication and Complication of Herbal MedicineДокумент26 страницHealth Implication and Complication of Herbal Medicineigweonyia gabrielОценок пока нет
- Nursing Care To Promote Fetal and Maternal HealthДокумент4 страницыNursing Care To Promote Fetal and Maternal HealthKristine BartsОценок пока нет
- Shoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesДокумент3 страницыShoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesSahithya MОценок пока нет
- The Role of The Microbiota in Periodontal DiseaseДокумент12 страницThe Role of The Microbiota in Periodontal DiseaseNishtha KumarОценок пока нет
- Definition and Characteristics.: Antibiosis, Which Means "Against Life," Was Introduced by The French BacteriologistДокумент4 страницыDefinition and Characteristics.: Antibiosis, Which Means "Against Life," Was Introduced by The French BacteriologistfirozbangladeshОценок пока нет
- CASE REPORT COMPETITION With Identifying FeaturesДокумент12 страницCASE REPORT COMPETITION With Identifying FeaturesJoel Cesar AtinadoОценок пока нет
- Bahasa Inggris - NurfadilahДокумент6 страницBahasa Inggris - NurfadilahHardianiОценок пока нет
- Silabus Rmo 2021Документ13 страницSilabus Rmo 2021Nuzlan NuariОценок пока нет
- 3927 9620 1 PBДокумент5 страниц3927 9620 1 PBdinul fitrati putriОценок пока нет
- Reflection Paper About Covid-19Документ1 страницаReflection Paper About Covid-19sei gosa100% (1)
- WT OetДокумент13 страницWT OetRomana PereiraОценок пока нет
- Burn Assessment CMU PDFДокумент2 страницыBurn Assessment CMU PDFmegamindОценок пока нет
- Mechanisms Case StudyДокумент13 страницMechanisms Case Studyshane_tin143Оценок пока нет
- Patient A (Click On The Link To "Complete Patient A's Karyotype")Документ2 страницыPatient A (Click On The Link To "Complete Patient A's Karyotype")ZzaiRraОценок пока нет
- Bllod Transfision ConsentДокумент1 страницаBllod Transfision ConsentumeshbhartiОценок пока нет
- Competency Statement Compliance Criteria Validation Method Validated by DateДокумент4 страницыCompetency Statement Compliance Criteria Validation Method Validated by DateRosalinda Manuel VigiliaОценок пока нет
- Freddie MercuryДокумент3 страницыFreddie MercuryBiju JosephОценок пока нет
- Perforasi Pada Penderita Apendisitis Di RSUD DR.H.Abdul Moeloek LampungДокумент7 страницPerforasi Pada Penderita Apendisitis Di RSUD DR.H.Abdul Moeloek LampungKikiОценок пока нет
- Form 86 2022 Health Examination RecordДокумент1 страницаForm 86 2022 Health Examination RecordMA. GLIZA TANОценок пока нет
- Cronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementДокумент4 страницыCronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementAnandhu GОценок пока нет
- Name of The Medicinal Product: Novaminsulfon Abz 500 MG/ML TropfenДокумент8 страницName of The Medicinal Product: Novaminsulfon Abz 500 MG/ML TropfenRiriОценок пока нет