Вам также может понравиться
- Productivity and Reliability-Based Maintenance Management, Second EditionОт EverandProductivity and Reliability-Based Maintenance Management, Second EditionОценок пока нет
- Study of Aspects of Data Quality - COMADEM International JournalДокумент13 страницStudy of Aspects of Data Quality - COMADEM International JournalMustafa IbrahimОценок пока нет
- Tensile TesterДокумент12 страницTensile Testerlhanx2Оценок пока нет
- Total Productive Maintenance (TPM)Документ14 страницTotal Productive Maintenance (TPM)RAM KUMARОценок пока нет
- Surface Vehicle StandardДокумент5 страницSurface Vehicle StandardLeonardo Gonçalves GomideОценок пока нет
- Acad98 004R1Документ66 страницAcad98 004R1michael1971Оценок пока нет
- Supply Chain Challenges - Mining IndustryДокумент2 страницыSupply Chain Challenges - Mining Industryshikhar19Оценок пока нет
- Weekly Piano Practice PlanДокумент2 страницыWeekly Piano Practice PlanKevin Jordan0% (1)
- 111equation Chapter 1 Section 1: Submitted: Dr. Awais SUBMITTED BY:2108-ME-85 Section BДокумент20 страниц111equation Chapter 1 Section 1: Submitted: Dr. Awais SUBMITTED BY:2108-ME-85 Section BFatima AsifОценок пока нет
- Planning For Avian Flu Disruptions On Global Operations A DMAIC Case StudyДокумент19 страницPlanning For Avian Flu Disruptions On Global Operations A DMAIC Case StudydrustagiОценок пока нет
- Cyclone Tracy Case StudyДокумент2 страницыCyclone Tracy Case StudyIrene XieОценок пока нет
- Reduce Reject Painting Process Using Six Sigma Method With Dmaic Approach and Experiments On Brake Disc Products (1 RC Hub) (Case Study in Pt. Xyz)Документ11 страницReduce Reject Painting Process Using Six Sigma Method With Dmaic Approach and Experiments On Brake Disc Products (1 RC Hub) (Case Study in Pt. Xyz)International Journal of Innovative Science and Research TechnologyОценок пока нет
- Enterprise Asset Management For Ports, TereminalsДокумент2 страницыEnterprise Asset Management For Ports, TereminalsAinyeéArwalyéОценок пока нет
- NDT MethodsДокумент2 страницыNDT MethodsSatya RaoОценок пока нет
- Analysis of Print Quality Control of Canned Materials With The DMAIC Method in PT United Can Company New Printing DepartmentДокумент6 страницAnalysis of Print Quality Control of Canned Materials With The DMAIC Method in PT United Can Company New Printing DepartmentInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- STM Keypad Design GuideДокумент35 страницSTM Keypad Design Guidesav33Оценок пока нет
- Industrial Engineering - Research Topics 2017Документ22 страницыIndustrial Engineering - Research Topics 2017rizwanooo0Оценок пока нет
- 2 How To Make A Pump Selection - Intro To PumpsДокумент7 страниц2 How To Make A Pump Selection - Intro To PumpsMohammed MustafaОценок пока нет
- Insulating Varnish TYPESДокумент26 страницInsulating Varnish TYPESJoeyPol PolancosОценок пока нет
- Fretting PDFДокумент8 страницFretting PDFRohan MalkarОценок пока нет
- Life Cycle Institute-SMRP BOK-Detailed Outline (2840)Документ3 страницыLife Cycle Institute-SMRP BOK-Detailed Outline (2840)jhonatan lorenzoОценок пока нет
- DFMДокумент4 страницыDFMMarko BrkicОценок пока нет
- Emaint X3 CMMS - GeneralДокумент33 страницыEmaint X3 CMMS - GeneralDon100% (2)
- Pages From Guidelines For The Management of Flexible Hose AssembliesДокумент2 страницыPages From Guidelines For The Management of Flexible Hose Assembliesjson_gabionОценок пока нет
- The Problem With Waiting TimeДокумент8 страницThe Problem With Waiting Timemano7428Оценок пока нет
- CMMS Technical Object and Preventative Maintenance FormДокумент7 страницCMMS Technical Object and Preventative Maintenance Formken1962Оценок пока нет
- MaptqДокумент3 страницыMaptqabisaad dimyatiОценок пока нет
- Advanced Diagnostics and Prognostics For Gas Turbine Engine Risk AssessmentДокумент10 страницAdvanced Diagnostics and Prognostics For Gas Turbine Engine Risk AssessmentВячеслав НадежкинОценок пока нет
- Danh Muc Cac Tieu Chuan IsoДокумент89 страницDanh Muc Cac Tieu Chuan IsoSocola MiMiОценок пока нет
- Oetiker ClampДокумент122 страницыOetiker ClampVennia PapadipoulouОценок пока нет
- White Paper Automated Ultrasonic Inspection of Tube To Tube Sheet WeldsДокумент7 страницWhite Paper Automated Ultrasonic Inspection of Tube To Tube Sheet WeldsdanemsalОценок пока нет
- TENTEC Hydraulic Ancillary Data Sheet R7 A4Документ4 страницыTENTEC Hydraulic Ancillary Data Sheet R7 A4Juliyan PujakesumaОценок пока нет
- Santoprene Blow Molding Guide EnpdfДокумент23 страницыSantoprene Blow Molding Guide EnpdfNikhil AherОценок пока нет
- Failure MechanismsДокумент14 страницFailure Mechanismsho-faОценок пока нет
- Is 14700 4 1 2008Документ20 страницIs 14700 4 1 2008Juan Pablo Villazon RichterОценок пока нет
- Flex Sim BrochureДокумент4 страницыFlex Sim BrochureArielovimagОценок пока нет
- Failure Analysis of Belt Conveyor SystemsДокумент17 страницFailure Analysis of Belt Conveyor SystemsGogyОценок пока нет
- Design For LogisticsДокумент22 страницыDesign For LogisticsBarun BhardwajОценок пока нет
- Notes To File Guidance 04-20-12Документ3 страницыNotes To File Guidance 04-20-12Sashwat TanayОценок пока нет
- 23) E-00-0800 - General Test Methods For Cold Impact Behavior On Automotive PlasoДокумент5 страниц23) E-00-0800 - General Test Methods For Cold Impact Behavior On Automotive PlasoShyam MehtaОценок пока нет
- Mapcon CMMS Feature ChartДокумент6 страницMapcon CMMS Feature ChartStar RangerОценок пока нет
- Supply-ChainДокумент61 страницаSupply-ChainJackson TeohОценок пока нет
- QEHS ALERT 15-XXX - Class II Welding Requirements R0 - ScribdДокумент2 страницыQEHS ALERT 15-XXX - Class II Welding Requirements R0 - ScribdLummersОценок пока нет
- Varnish - Chemistry 2Документ4 страницыVarnish - Chemistry 2Akshat GoyalОценок пока нет
- Fretting SolutionДокумент8 страницFretting SolutionRohan MalkarОценок пока нет
- MC117 PipingFailuresДокумент3 страницыMC117 PipingFailuresshakeelahmadjsrОценок пока нет
- Welding Is AДокумент15 страницWelding Is Avijayans_1Оценок пока нет
- Approval of Electrical Equipment Information Booklet 2014-18 Mac 2015Документ72 страницыApproval of Electrical Equipment Information Booklet 2014-18 Mac 2015Anonymous N66xkZiZ6g100% (1)
- A Review On Condition-Based Maintenance Optimization Models For Stochastically Deteriorating SystemДокумент42 страницыA Review On Condition-Based Maintenance Optimization Models For Stochastically Deteriorating SystemCESARALARCON1Оценок пока нет
- Case StudyДокумент6 страницCase StudyelectronicssucksОценок пока нет
- Reliability Centred Maintenance Shivajichoudhury DownloadДокумент4 страницыReliability Centred Maintenance Shivajichoudhury DownloadNantha KumarОценок пока нет
- Deposition of Stellite 6 Hard Facing OveДокумент44 страницыDeposition of Stellite 6 Hard Facing OveDat GreenОценок пока нет
- 03 Ppap-3 PDFДокумент91 страница03 Ppap-3 PDFMalla Reddy AVОценок пока нет
- A R C H I V e o F S I D Maintenance Management Decision Model For Preventive Maintenance Strategy On Production EquipmentДокумент14 страницA R C H I V e o F S I D Maintenance Management Decision Model For Preventive Maintenance Strategy On Production EquipmentLASER LION100% (1)
- Failure AnalysisДокумент23 страницыFailure AnalysisMaruan MuhammadОценок пока нет
- Welding PlasticsДокумент22 страницыWelding Plasticssav33Оценок пока нет
- LayoutДокумент5 страницLayoutPrem RanjanОценок пока нет
- Powder CoatingsДокумент30 страницPowder Coatingsferdlh9Оценок пока нет
- Corrosion Swimming)Документ6 страницCorrosion Swimming)skenny1Оценок пока нет
- Acw 0219Документ2 страницыAcw 0219anna_malai078351Оценок пока нет
- Repertoire List: Date Title of Piece ComposerДокумент1 страницаRepertoire List: Date Title of Piece ComposerKevin JordanОценок пока нет
- Table Design WorksheetДокумент1 страницаTable Design WorksheetKevin JordanОценок пока нет
- Weekly Guitar Practice PlanДокумент1 страницаWeekly Guitar Practice PlanKevin Jordan100% (2)
- KNVB Coaching Corner 1pdfДокумент2 страницыKNVB Coaching Corner 1pdfKevin Jordan100% (1)
- U.S. Soccer "D" License Course Candidate Manual How To Run A PracticeДокумент11 страницU.S. Soccer "D" License Course Candidate Manual How To Run A PracticeKevin JordanОценок пока нет
- Coaching Manual: 60 Shooting PracticeДокумент1 страницаCoaching Manual: 60 Shooting PracticeKevin JordanОценок пока нет
- Coaching Manual: Possession FootballДокумент1 страницаCoaching Manual: Possession FootballKevin JordanОценок пока нет
- Coaching Manual: Small-Sided DrillДокумент1 страницаCoaching Manual: Small-Sided DrillKevin JordanОценок пока нет
- Coaching Manual: Goalkeepers: Crosses & DistributionДокумент1 страницаCoaching Manual: Goalkeepers: Crosses & DistributionKevin JordanОценок пока нет
- Coaching Manual: Crossing From The Wide ZoneДокумент1 страницаCoaching Manual: Crossing From The Wide ZoneKevin JordanОценок пока нет
- Coaching Manual: 59 Attacking Two GoalsДокумент1 страницаCoaching Manual: 59 Attacking Two GoalsKevin JordanОценок пока нет
- Mobile Robots and Autonomous VehiclesДокумент2 страницыMobile Robots and Autonomous VehiclesAbel Varghese DavidОценок пока нет
- Biochemical Oxygen DemandДокумент18 страницBiochemical Oxygen DemandUnputdownable Bishwarup100% (1)
- Color Code - Canadian Standard - ABES - PROD.PW - MC.B017.E24806.ATTA003Документ14 страницColor Code - Canadian Standard - ABES - PROD.PW - MC.B017.E24806.ATTA003Adam Michael GreenОценок пока нет
- Cummins ECM Reference NotesДокумент11 страницCummins ECM Reference NotesjuanОценок пока нет
- TIA Workshop ITBДокумент48 страницTIA Workshop ITBFirman Suhendra100% (1)
- Case StudyДокумент2 страницыCase StudyAyeng 1502100% (1)
- Electrical Load For Indoor UnitsДокумент2 страницыElectrical Load For Indoor UnitsMD BILAL ASLAMОценок пока нет
- System Failure AnalysisДокумент9 страницSystem Failure AnalysisHermance Yosepf Setiarto Harimurti50% (2)
- ABB Wireless Communications For Mining OperationsДокумент38 страницABB Wireless Communications For Mining OperationsAymanОценок пока нет
- CCR Equipment ListДокумент1 страницаCCR Equipment Listbehzad parsiОценок пока нет
- Turning Circles and Stopping DistancesДокумент7 страницTurning Circles and Stopping DistancesBisrat100% (1)
- BUT11F/11AF: NPN Silicon TransistorДокумент4 страницыBUT11F/11AF: NPN Silicon TransistorfabioboogОценок пока нет
- Global Deduplication Array Administration Guide: DD OS 5.0Документ70 страницGlobal Deduplication Array Administration Guide: DD OS 5.0Rajesh KumarОценок пока нет
- NDT NablДокумент3 страницыNDT NablPrabir KumarОценок пока нет
- TDS 9-11SA Mechanical TroubleshootingДокумент34 страницыTDS 9-11SA Mechanical Troubleshootingahmed.kareem.khanjerОценок пока нет
- Workover Kill Fluid Density CalculationДокумент3 страницыWorkover Kill Fluid Density CalculationSanny Astari100% (1)
- Eminence Deltalite II 2515Документ1 страницаEminence Deltalite II 2515Suto BandОценок пока нет
- Experience The Latest & Safest in Building Circuit ProtectionДокумент28 страницExperience The Latest & Safest in Building Circuit ProtectionYashwanth KrishnanОценок пока нет
- Trodat Standard Self Inking Stamp and Accessory Mini CatalogДокумент12 страницTrodat Standard Self Inking Stamp and Accessory Mini CatalogpromotesourceОценок пока нет
- Rescue Boat Lsa 5.1Документ4 страницыRescue Boat Lsa 5.1Celal BozdoganОценок пока нет
- Banumathy.D Updated Profile 1Документ7 страницBanumathy.D Updated Profile 1engineeringwatchОценок пока нет
- Fire Protection Engineering Summer 2001Документ33 страницыFire Protection Engineering Summer 2001Hany RifaatОценок пока нет
- Fis-Opf Ach PaymentsДокумент5 страницFis-Opf Ach PaymentscrazytrainОценок пока нет
- 6.hydraulic Pressure SpesificationДокумент3 страницы6.hydraulic Pressure SpesificationTLK ChannelОценок пока нет
- Physics 23 Fall 1993 Lab 2 - Adiabatic Processes: PV NRTДокумент13 страницPhysics 23 Fall 1993 Lab 2 - Adiabatic Processes: PV NRTvipul ch v v n s sОценок пока нет
- Whirlpool SPIW318A2WF Air ConditionerДокумент324 страницыWhirlpool SPIW318A2WF Air ConditionerAxxОценок пока нет
- GEK 116403 Ge File. Performance TestsДокумент54 страницыGEK 116403 Ge File. Performance TestsSulaiman JafferyОценок пока нет
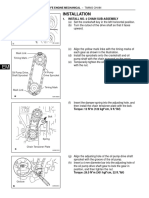
- Sincronizacion de Motor Toyota 2az-FeДокумент12 страницSincronizacion de Motor Toyota 2az-FeWilliams NavasОценок пока нет
- NR 10 Specification 75AДокумент2 страницыNR 10 Specification 75AHsalmani1991Оценок пока нет
- Image AnalysisДокумент404 страницыImage Analysisholyfreeman34Оценок пока нет