Вам также может понравиться
- Receipt: in Respect of Payment of Registration Fee For Event ListedДокумент2 страницыReceipt: in Respect of Payment of Registration Fee For Event ListedUday PrabhuОценок пока нет
- Dips BrochureДокумент2 страницыDips BrochureUday PrabhuОценок пока нет
- Core Topics in General & Emergency SurgeryДокумент75 страницCore Topics in General & Emergency SurgeryUday PrabhuОценок пока нет
- Systematic Review of The Prevalence of Faecal IncontinenceДокумент9 страницSystematic Review of The Prevalence of Faecal IncontinenceUday PrabhuОценок пока нет
- QPДокумент2 страницыQPUday PrabhuОценок пока нет
- RCT AntibioticsДокумент8 страницRCT AntibioticsUday PrabhuОценок пока нет
- Meta-Analysis of Closure of The Fascial Defect During Laparoscopic Incisional and Ventral Hernia RepairДокумент10 страницMeta-Analysis of Closure of The Fascial Defect During Laparoscopic Incisional and Ventral Hernia RepairUday PrabhuОценок пока нет
- Surg 1015 501Документ8 страницSurg 1015 501Uday PrabhuОценок пока нет
- Core Topics in General & Emergency SurgeryДокумент75 страницCore Topics in General & Emergency SurgeryUday PrabhuОценок пока нет
- Bjs 10289Документ10 страницBjs 10289Uday PrabhuОценок пока нет
- Guidance Venous Thromboembolism Reducing The Risk PDFДокумент57 страницGuidance Venous Thromboembolism Reducing The Risk PDFUday PrabhuОценок пока нет
- Thoracic Injury Management Jan 08Документ39 страницThoracic Injury Management Jan 08Uday PrabhuОценок пока нет
- Cost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationДокумент10 страницCost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationUday PrabhuОценок пока нет
- Giant Inguinal Hernia: A Case ReportДокумент5 страницGiant Inguinal Hernia: A Case ReportUday PrabhuОценок пока нет
- Cost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationДокумент10 страницCost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationUday PrabhuОценок пока нет
- CM1 M.H.DavisДокумент7 страницCM1 M.H.DavisUday PrabhuОценок пока нет
- CD 008674Документ28 страницCD 008674Uday PrabhuОценок пока нет
- PowerДокумент41 страницаPowerLuis PenuttОценок пока нет
- Statistical Test Power Bone Mineral StudyДокумент8 страницStatistical Test Power Bone Mineral Studymathan_de_rockОценок пока нет
- Head and NeckДокумент21 страницаHead and NeckUday PrabhuОценок пока нет
- Remote and Rural SurgeryДокумент12 страницRemote and Rural SurgeryUday PrabhuОценок пока нет
- OesophagusДокумент32 страницыOesophagusUday PrabhuОценок пока нет
- Genitourinary SurgeryДокумент14 страницGenitourinary SurgeryUday PrabhuОценок пока нет
- The Adrenal GlandsДокумент10 страницThe Adrenal GlandsUday PrabhuОценок пока нет
- S 11Документ2 страницыS 11Uday PrabhuОценок пока нет
- Last Moment ReviseДокумент1 страницаLast Moment ReviseUday PrabhuОценок пока нет
- The Parathyroid GlandsДокумент7 страницThe Parathyroid GlandsUday PrabhuОценок пока нет
- Basic Medical Statistics (Definitions)Документ3 страницыBasic Medical Statistics (Definitions)ChristopherMcMasterОценок пока нет
- Harun FRCS Journey Tips1Документ4 страницыHarun FRCS Journey Tips1Uday Prabhu50% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Revocation of Wills Case DigestsДокумент3 страницыRevocation of Wills Case DigestsArgel Joseph CosmeОценок пока нет
- How Social Influence Impacts Consumer BehaviorДокумент31 страницаHow Social Influence Impacts Consumer BehaviorayeshasarafОценок пока нет
- Paediatrics MCQ PointsДокумент117 страницPaediatrics MCQ PointstharikaneelawathuraОценок пока нет
- Gomez FL Bar Complaint v. PerezДокумент6 страницGomez FL Bar Complaint v. PerezJudgeHSОценок пока нет
- Learn Prepositions and ArticlesДокумент12 страницLearn Prepositions and ArticlesAl-Ami SarkerОценок пока нет
- Value Delivery Bucket ListДокумент31 страницаValue Delivery Bucket ListLuis Carlos ChacónОценок пока нет
- Schizophrenia Concept MapДокумент3 страницыSchizophrenia Concept Mapsammillepointer86Оценок пока нет
- Supply Chain of MilkДокумент6 страницSupply Chain of MilkFahad TatlaОценок пока нет
- CHAPTER VI CREATING BRAND EQUITY - Manansala - RolynДокумент16 страницCHAPTER VI CREATING BRAND EQUITY - Manansala - RolynROLYNОценок пока нет
- Branton - The Dulce Book PDFДокумент433 страницыBranton - The Dulce Book PDFnityapriya.meОценок пока нет
- 14 Tantoco v. Municipal Council - DigestДокумент1 страница14 Tantoco v. Municipal Council - DigestAbigail TolabingОценок пока нет
- Measurement of Financial LiabilitiesДокумент8 страницMeasurement of Financial Liabilitiesjoyce KimОценок пока нет
- Color Techniques for Landscape DesignДокумент11 страницColor Techniques for Landscape Designgildesenganio100% (1)
- Emergent Reader Case Summary SheetДокумент2 страницыEmergent Reader Case Summary Sheetapi-503192153Оценок пока нет
- Factors Forcing Children To Street Hargeissa, SomalilandДокумент4 страницыFactors Forcing Children To Street Hargeissa, SomalilandInternational Journal of Innovative Science and Research Technology100% (2)
- Flower Structure and FunctionДокумент3 страницыFlower Structure and Functionwafwfw0% (1)
- Answer Key Perfect ScoreДокумент4 страницыAnswer Key Perfect ScoreainsaadahОценок пока нет
- Crossing The Waves of Ecocriticism: Living During The AnthropoceneДокумент2 страницыCrossing The Waves of Ecocriticism: Living During The AnthropoceneMuHammAD ShArjeeLОценок пока нет
- West Gate Tunnel Project AgreementДокумент1 465 страницWest Gate Tunnel Project AgreementBilly LeeОценок пока нет
- Clmo-11 Gyratory Sieve ShakerДокумент4 страницыClmo-11 Gyratory Sieve ShakerErGiteshAroraОценок пока нет
- Physical Chemical Changes Lesson 2 ReflectionДокумент2 страницыPhysical Chemical Changes Lesson 2 Reflectionapi-360585476Оценок пока нет
- Criminal Incident Report FF-560-302Документ3 страницыCriminal Incident Report FF-560-302David100% (1)
- Distraction Techniques Reduce Pain in Children During Medical ProceduresДокумент7 страницDistraction Techniques Reduce Pain in Children During Medical ProceduresTuti NingsihОценок пока нет
- Changing The World of Dentistry With Dental InformaticsДокумент49 страницChanging The World of Dentistry With Dental InformaticsTitus SchleyerОценок пока нет
- Recognition Day 2023 - Bartolabac-Straight FeatureДокумент3 страницыRecognition Day 2023 - Bartolabac-Straight FeatureAnne BartolabacОценок пока нет
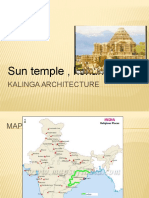
- Konark Sun Temple, a 13th century architectural marvelДокумент18 страницKonark Sun Temple, a 13th century architectural marvelSyed Ahmed KabeerОценок пока нет
- FUJITSU 1.2GHz PLL Frequency Synthesizer Data SheetДокумент26 страницFUJITSU 1.2GHz PLL Frequency Synthesizer Data SheetherzvaiОценок пока нет
- Levator Ani SyndromeДокумент24 страницыLevator Ani SyndromeKavya KavyasujathaОценок пока нет
- Secured Transactions Torts and Damages Preference of Credits Examination QuestionsДокумент14 страницSecured Transactions Torts and Damages Preference of Credits Examination QuestionsPilacan KarylОценок пока нет
- Julian RzoskaДокумент409 страницJulian RzoskaPietro FuscoОценок пока нет