Вам также может понравиться
- Associations Between Sleep Problems, Anxiety, and Depression in Twins at 8 Years of AgeДокумент10 страницAssociations Between Sleep Problems, Anxiety, and Depression in Twins at 8 Years of AgeICU RSUNSОценок пока нет
- ArticleДокумент6 страницArticleHerbert Baquerizo VargasОценок пока нет
- Psychiatry ResearchДокумент9 страницPsychiatry ResearchAlberto RicoОценок пока нет
- Aindev 2012 12 004Документ10 страницAindev 2012 12 004Gisele Elise MeninОценок пока нет
- Me Lend Res 2004Документ8 страницMe Lend Res 2004Viris MartínezОценок пока нет
- ADHD ID Family StudyДокумент27 страницADHD ID Family StudyStephen FaraoneОценок пока нет
- Mellon2013 PDFДокумент22 страницыMellon2013 PDFSipi SomOfОценок пока нет
- 1 s2.0 S1087079213000440 MainДокумент13 страниц1 s2.0 S1087079213000440 Mainm67arthaОценок пока нет
- Poor Sleep and Altered Hypothalamic-Pituitary-Adrenocortical and Sympatho-Adrenal-Medullary System Activity in ChildrenДокумент8 страницPoor Sleep and Altered Hypothalamic-Pituitary-Adrenocortical and Sympatho-Adrenal-Medullary System Activity in Childrenapi-25984288Оценок пока нет
- Desta Actaped 2006 PDFДокумент5 страницDesta Actaped 2006 PDFyohanesОценок пока нет
- Research in Developmental DisabilitiesДокумент9 страницResearch in Developmental DisabilitiesRafael MartinsОценок пока нет
- Research in Developmental Disabilities: J. Keating, J. Bramham, M. DownesДокумент13 страницResearch in Developmental Disabilities: J. Keating, J. Bramham, M. DownesBotez MartaОценок пока нет
- Robinson2012 Article ChildhoodEpilepsyAndAutismSpecДокумент9 страницRobinson2012 Article ChildhoodEpilepsyAndAutismSpecTheo KhouryОценок пока нет
- Childhood Onset Schizophrenia High Rate of Visual HallucinationsДокумент9 страницChildhood Onset Schizophrenia High Rate of Visual HallucinationsmiaaОценок пока нет
- Research in Autism Spectrum DisordersДокумент9 страницResearch in Autism Spectrum DisorderspsicosmosОценок пока нет
- Epilepsy and BehaviorДокумент8 страницEpilepsy and Behaviorviviana84Оценок пока нет
- Sleep Medicine: Salvatore P. Insana, David Gozal, Daniel W. Mcneil, Hawley E. Montgomery-DownsДокумент6 страницSleep Medicine: Salvatore P. Insana, David Gozal, Daniel W. Mcneil, Hawley E. Montgomery-DownsMuhammad ArifОценок пока нет
- Sleep Habits and Disturbances in Malaysian Children With EpilepsyДокумент5 страницSleep Habits and Disturbances in Malaysian Children With EpilepsynoiОценок пока нет
- 2019, Merlo e Briley, Problemas Do Sono Na Criança Que GaguejaДокумент11 страниц2019, Merlo e Briley, Problemas Do Sono Na Criança Que GaguejaCarol PaesОценок пока нет
- Iq in Epilepsy.2013.07.010Документ6 страницIq in Epilepsy.2013.07.010thelegend 2022Оценок пока нет
- Pzab 177Документ10 страницPzab 177LORENZO GABRIEL BANAYOОценок пока нет
- Factor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisДокумент9 страницFactor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisCris RodriguesОценок пока нет
- Application of The Sleep Disturbance Scale For Children (SDSC) in Preschool AgeДокумент9 страницApplication of The Sleep Disturbance Scale For Children (SDSC) in Preschool AgeerikafebriyanarОценок пока нет
- Goldman 2011Документ7 страницGoldman 2011Angie ValenciaОценок пока нет
- See AnotherДокумент7 страницSee AnothercathyОценок пока нет
- Báo 5Документ9 страницBáo 5Thanh Nhàn Nguyễn ThịОценок пока нет
- Sleep Interventions For Children With Attention Deficit Hyperactivity Disorder (ADHD) : A Systematic Literature ReviewДокумент12 страницSleep Interventions For Children With Attention Deficit Hyperactivity Disorder (ADHD) : A Systematic Literature ReviewRamacil Afsan NotoprawiroОценок пока нет
- Neurodevelopmental Outcomes of Preterm Infants: A Recent Literature ReviewДокумент6 страницNeurodevelopmental Outcomes of Preterm Infants: A Recent Literature ReviewJyotirmayeeОценок пока нет
- Kozeis 2007 - Visual Function and Visual Perception in Cerebral Palsied ChildrenДокумент11 страницKozeis 2007 - Visual Function and Visual Perception in Cerebral Palsied Childrenangeles sanchez clariaОценок пока нет
- CraniomanuscriptV3revisedmanuscript ForresearchgateДокумент19 страницCraniomanuscriptV3revisedmanuscript ForresearchgatefelitaОценок пока нет
- Incidence of Pre-Peri and Post-Natal Developmental Factors - FrontiersДокумент12 страницIncidence of Pre-Peri and Post-Natal Developmental Factors - FrontiersfernandaОценок пока нет
- Preventive Medicine: Jennifer I. Gapin, Jeffrey D. Labban, Jennifer L. EtnierДокумент5 страницPreventive Medicine: Jennifer I. Gapin, Jeffrey D. Labban, Jennifer L. EtnierrobfoxОценок пока нет
- Behavioral InterventionsДокумент13 страницBehavioral Interventionsbmunir2Оценок пока нет
- 2018 - Adhd e VLBWДокумент18 страниц2018 - Adhd e VLBWdeborahpreitiОценок пока нет
- Sueño 2Документ13 страницSueño 2Evelyn Esther Díaz HarosОценок пока нет
- Factors in Uencing Excessive Daytime Sleepiness in AdolescentsДокумент7 страницFactors in Uencing Excessive Daytime Sleepiness in AdolescentsRenata YolandaОценок пока нет
- Autism Spectrum Disorders in Extremely Preterm Children OriginalДокумент9 страницAutism Spectrum Disorders in Extremely Preterm Children Originalesteban_falcón_12Оценок пока нет
- Jurnal Down Syndrome (Eriza Eka Patrisia 21123028P)Документ8 страницJurnal Down Syndrome (Eriza Eka Patrisia 21123028P)yfbppqcvhtОценок пока нет
- The Assessment of ADHD in Persons With Developmental DisabilitiesДокумент24 страницыThe Assessment of ADHD in Persons With Developmental DisabilitiesCristina0% (1)
- Content ServerДокумент11 страницContent ServerhafiezAmandaОценок пока нет
- A National Profile of Childhood Epilepsy and Seizure DisorderДокумент11 страницA National Profile of Childhood Epilepsy and Seizure DisorderYovan FabianОценок пока нет
- Prevalence of Sleep Disorder 1 (Y.2010)Документ17 страницPrevalence of Sleep Disorder 1 (Y.2010)Siti Lestari RemantoОценок пока нет
- Ms Proposal GLD ArtifactДокумент3 страницыMs Proposal GLD Artifactapi-505989771Оценок пока нет
- E541 FullДокумент9 страницE541 FullAlba VilaОценок пока нет
- El Sheikh - Sleep and Disparities in Child and Adolescent DevelopmentДокумент8 страницEl Sheikh - Sleep and Disparities in Child and Adolescent DevelopmentLilianneОценок пока нет
- Research Submission: Primary Headache and Sleep Disturbances in AdolescentsДокумент6 страницResearch Submission: Primary Headache and Sleep Disturbances in AdolescentsAghie vlogОценок пока нет
- Peds 2012-0900IДокумент19 страницPeds 2012-0900IAsma Ayad GhaziОценок пока нет
- Developmental Neuropsychology PreprintversionДокумент48 страницDevelopmental Neuropsychology PreprintversionHijaz HijaОценок пока нет
- CSHQДокумент11 страницCSHQRiffq Rambu AnarkiОценок пока нет
- Impact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenДокумент10 страницImpact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenEunice_Pinto_1725Оценок пока нет
- Mama SelinДокумент4 страницыMama SelinIndah LakataraОценок пока нет
- Development of Bipolar Disorder and Other Comorbilities en TDAHДокумент7 страницDevelopment of Bipolar Disorder and Other Comorbilities en TDAHCarla NapoliОценок пока нет
- Journal Adhi DR Rini Behavioral Problems in Children With Epilepsy (Autosaved)Документ33 страницыJournal Adhi DR Rini Behavioral Problems in Children With Epilepsy (Autosaved)Utomo SiswoОценок пока нет
- Cognitive Impact in Children With Benign Childhood Focal Epilepsy WithДокумент4 страницыCognitive Impact in Children With Benign Childhood Focal Epilepsy WithHeldice MachadoОценок пока нет
- Journal Pedsos MadyaДокумент9 страницJournal Pedsos MadyaHajrin PajriОценок пока нет
- Behavior Problems in Children of Parents With Anxiety DisordersДокумент6 страницBehavior Problems in Children of Parents With Anxiety DisordersRaquel de Azevedo de SouzaОценок пока нет
- Developmental Correlates Persistent Snoring in Preschool Children: Predictors and Behavioral andДокумент10 страницDevelopmental Correlates Persistent Snoring in Preschool Children: Predictors and Behavioral andsambalikadzilla6052Оценок пока нет
- Feeding Proem.xДокумент4 страницыFeeding Proem.xMuhammad Yusril JalilОценок пока нет
- Serial Developmental Assessments in Infants With Deformational Plagiocephalyjpc - 2234 274..278Документ5 страницSerial Developmental Assessments in Infants With Deformational Plagiocephalyjpc - 2234 274..278chiaraОценок пока нет
- Diagnosis and Treatment of Children With Autism Spectrum DisordersОт EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersРейтинг: 5 из 5 звезд5/5 (1)
- Asia-Pacific Glaucoma Guidelines PDFДокумент118 страницAsia-Pacific Glaucoma Guidelines PDFAvilla Ane LukitoОценок пока нет
- Jay W. Marks, M.D. Dennis Lee, M.D. Bile Liver: GallstonesДокумент11 страницJay W. Marks, M.D. Dennis Lee, M.D. Bile Liver: GallstonesAvilla Ane LukitoОценок пока нет
- Simple Jul04 A4Документ1 страницаSimple Jul04 A4Avilla Ane LukitoОценок пока нет
- Corneal Sensitivity and Dry Eye Symptoms in Patients With KeratoconusДокумент12 страницCorneal Sensitivity and Dry Eye Symptoms in Patients With KeratoconusAvilla Ane LukitoОценок пока нет
- AZ ACOG Antepartum RecordДокумент6 страницAZ ACOG Antepartum RecordAvilla Ane LukitoОценок пока нет
- AZ ACOG Antepartum RecordДокумент6 страницAZ ACOG Antepartum RecordAvilla Ane LukitoОценок пока нет
- Literature Review-2Документ3 страницыLiterature Review-2api-500775510Оценок пока нет
- The Importance of Physical Fitness ExerciseДокумент4 страницыThe Importance of Physical Fitness ExercisePhilander FloresОценок пока нет
- Diabetes Prevention: 5 Tips For Taking Control: 1. Get More Physical ActivityДокумент2 страницыDiabetes Prevention: 5 Tips For Taking Control: 1. Get More Physical Activitymatindi galawanОценок пока нет
- 5.05 Don't Hold Your BreathДокумент5 страниц5.05 Don't Hold Your BreathSummer BОценок пока нет
- Protein Energy MalnutritionДокумент44 страницыProtein Energy Malnutritionokwadha simionОценок пока нет
- Full Download Introduction To Food Science and Food Systems 2nd Edition Parker Test BankДокумент35 страницFull Download Introduction To Food Science and Food Systems 2nd Edition Parker Test Bankbroomheadroseann708100% (34)
- Topic 7 Cardiorespiratory Adaptations To TrainingДокумент26 страницTopic 7 Cardiorespiratory Adaptations To TrainingCikguAmelia100% (1)
- Risk Assessment TemplateДокумент3 страницыRisk Assessment TemplateskiersteveОценок пока нет
- Status of Solid Waste Management in DelhipdfДокумент10 страницStatus of Solid Waste Management in DelhipdfShivang AgarwalОценок пока нет
- Eating Disorder StatisticsДокумент2 страницыEating Disorder Statisticsרוברטו מורןОценок пока нет
- Shelbey Hunter NutritionДокумент4 страницыShelbey Hunter Nutritionapi-548862372Оценок пока нет
- Brad Pilon Anabolic Again 2.0Документ227 страницBrad Pilon Anabolic Again 2.0karlos100% (4)
- How Often Do You Stay Up Late?: If You Don't Dream, You're Probably A Little CrazyДокумент16 страницHow Often Do You Stay Up Late?: If You Don't Dream, You're Probably A Little CrazyHelder BalantaОценок пока нет
- Republic Boliavarian of Venezuela University National Experimental "Simon Rodriguez" Nucleus MaturínДокумент10 страницRepublic Boliavarian of Venezuela University National Experimental "Simon Rodriguez" Nucleus MaturínYaritzaParraОценок пока нет
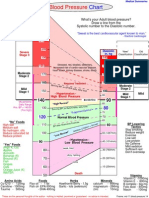
- Blood Pressure ChartДокумент1 страницаBlood Pressure ChartKAKKAMPI94% (16)
- OCR PE Recovery ProcessДокумент2 страницыOCR PE Recovery ProcessGeorge NoorlandОценок пока нет
- PE GROUP 4 REPORT Principles of Training FITT PrincipleДокумент27 страницPE GROUP 4 REPORT Principles of Training FITT PrincipleKristel May SomeraОценок пока нет
- Strings & Things Cheestrings Cheese Snack x8 160g Sainsbury'sДокумент1 страницаStrings & Things Cheestrings Cheese Snack x8 160g Sainsbury'sV1OОценок пока нет
- Strength Training Fundamentals in GymnasticsДокумент14 страницStrength Training Fundamentals in Gymnasticshavenoname9999100% (3)
- Irada 11 Ipa 6 PPT Hortatory ExpositionДокумент10 страницIrada 11 Ipa 6 PPT Hortatory ExpositionIradariva IradarivaОценок пока нет
- Meal Planning 1Документ12 страницMeal Planning 1KHALEEL SALEHОценок пока нет
- ScheduleДокумент2 страницыScheduleMax SaubermanОценок пока нет
- POT Lesson PlanДокумент4 страницыPOT Lesson PlanMichelle ThereseОценок пока нет
- Progressive OverloadДокумент23 страницыProgressive OverloadJohn Paul SarainОценок пока нет
- ASMI Safety AlertДокумент2 страницыASMI Safety AlertThillai8975Оценок пока нет
- LifestyleДокумент32 страницыLifestyleMidz SalipОценок пока нет
- TASK 1 (A)Документ13 страницTASK 1 (A)double keatОценок пока нет
- Health Is WealthДокумент1 страницаHealth Is Wealthriana safrianiОценок пока нет
- Henry D. Solatorio Jr. NCM 105: Promote Good Blood Sugar (Glucose) LevelsДокумент2 страницыHenry D. Solatorio Jr. NCM 105: Promote Good Blood Sugar (Glucose) LevelsCristoper BodionganОценок пока нет