Вам также может понравиться
- Shivani PDFДокумент3 страницыShivani PDFdeepukumarОценок пока нет
- Ulcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandUlcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- UTI GuidelineДокумент10 страницUTI Guidelinecatalin petreОценок пока нет
- Adult Infectious Disease Bulletpoints HandbookОт EverandAdult Infectious Disease Bulletpoints HandbookРейтинг: 4.5 из 5 звезд4.5/5 (9)
- Urinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideДокумент5 страницUrinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideLaoMed plusОценок пока нет
- UTI Guideline Example 2 Appendix B PDFДокумент4 страницыUTI Guideline Example 2 Appendix B PDFamira catriОценок пока нет
- Gamutin Drug Study-PediatricsДокумент6 страницGamutin Drug Study-PediatricsJhulia GamutinОценок пока нет
- Generic NameДокумент8 страницGeneric Namemel aquinoОценок пока нет
- Urinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of MedicineДокумент25 страницUrinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of Medicineولاء إبراهيمОценок пока нет
- Infeksi Saluran Kemih: Oleh Hendra Santoso Pembimbing Dr. Hasnawaty SP - OGДокумент22 страницыInfeksi Saluran Kemih: Oleh Hendra Santoso Pembimbing Dr. Hasnawaty SP - OGHendra SantosoОценок пока нет
- UTI Treatment Algorithm - Sharp Mesa Vista 2Документ3 страницыUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997Оценок пока нет
- Acute Uncomplicated PyelonephritisДокумент5 страницAcute Uncomplicated PyelonephritisoreaОценок пока нет
- UTI TreatmentДокумент3 страницыUTI TreatmentMaria RezitadinaОценок пока нет
- BCCA AB in Febrile Neutropenia GuidelinesДокумент2 страницыBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieОценок пока нет
- Urological InfectionsДокумент21 страницаUrological Infections<_>Оценок пока нет
- Urinary Tract Infections (UTI) in Older Adults WWW - Rxfiles.caДокумент7 страницUrinary Tract Infections (UTI) in Older Adults WWW - Rxfiles.caAwais KhanОценок пока нет
- Zinnat PIДокумент10 страницZinnat PIfsdfОценок пока нет
- UTI in ElderlyДокумент18 страницUTI in ElderlyBarkahafrilian100% (1)
- Literature Review On UTIДокумент31 страницаLiterature Review On UTINishchal Dhakal0% (1)
- 17 Urological InfectionsДокумент18 страниц17 Urological InfectionsntadudulОценок пока нет
- Pathophysiology of Pyelonephritis: How It HappensДокумент6 страницPathophysiology of Pyelonephritis: How It HappensReno Jun NagasanОценок пока нет
- Malaria and LeptospirosisДокумент18 страницMalaria and LeptospirosisRasYa DIОценок пока нет
- Uti TreatmentДокумент4 страницыUti TreatmentAnne OhОценок пока нет
- Antibiotka PicuДокумент4 страницыAntibiotka Picusunu rachmat100% (1)
- Antibiotik Dan Antiseptik Saluran KemihДокумент29 страницAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiОценок пока нет
- IMG EmpAposterДокумент1 страницаIMG EmpAposterChiu LeoОценок пока нет
- Cefuroxime Inhibits Bacterial Cell Wall Synthesis by Binding To One 1 or More of The Penicillin-Binding Proteins (PBPS) WhichДокумент12 страницCefuroxime Inhibits Bacterial Cell Wall Synthesis by Binding To One 1 or More of The Penicillin-Binding Proteins (PBPS) WhichMr rawrОценок пока нет
- Comprehension of Acute PyelonephritisДокумент23 страницыComprehension of Acute PyelonephritisAmeliaОценок пока нет
- Comprehension of Acute PyelonephritisДокумент23 страницыComprehension of Acute PyelonephritisAmeliaОценок пока нет
- ErythromycinДокумент2 страницыErythromycinBtob meloОценок пока нет
- University of Maryland Medical Center Fluconazole (Diflucan®)Документ6 страницUniversity of Maryland Medical Center Fluconazole (Diflucan®)damondouglasОценок пока нет
- Urinary Tract InfectionДокумент24 страницыUrinary Tract InfectionZaki Achmad NhrОценок пока нет
- Treatment of Urinary Tract Infections PDFДокумент24 страницыTreatment of Urinary Tract Infections PDFGoutham MОценок пока нет
- Pharmacotherapy of Urinary Tract InfectionДокумент75 страницPharmacotherapy of Urinary Tract InfectionMariana CreciunОценок пока нет
- NCLEX REVIEW AntibioticsДокумент7 страницNCLEX REVIEW Antibioticsneonstar100% (1)
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyДокумент20 страницAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019Оценок пока нет
- Treatment PDFДокумент6 страницTreatment PDFWorku KifleОценок пока нет
- Urinary Tract InfectionsДокумент28 страницUrinary Tract Infectionsleensaeed26Оценок пока нет
- Sepsis GuidelinesДокумент1 страницаSepsis GuidelinesYezenashОценок пока нет
- Ceftriaxone Drug StudyДокумент1 страницаCeftriaxone Drug StudyEsmareldah Henry SirueОценок пока нет
- Hello Everyone: Prof. (DR.) Akhilesh ShrivastavaДокумент19 страницHello Everyone: Prof. (DR.) Akhilesh Shrivastavaarpitagupta28Оценок пока нет
- EAU Pocket Guidelines On Urological Infections 2021Документ25 страницEAU Pocket Guidelines On Urological Infections 2021Noel Saúl Argüello SánchezОценок пока нет
- Patients With Multiple DisordersДокумент7 страницPatients With Multiple DisordersKathleen Joy PingenОценок пока нет
- Eau Guidelines On Urological Infections: (Limited Text Update March 2020)Документ22 страницыEau Guidelines On Urological Infections: (Limited Text Update March 2020)LUIS MIGUEL CASTILLA MORANОценок пока нет
- Name of Drug: Ceftriaxone 2g/IVДокумент3 страницыName of Drug: Ceftriaxone 2g/IVAllan DiazОценок пока нет
- Antibiotic Policy JIPMER UTIДокумент6 страницAntibiotic Policy JIPMER UTIRpmhouseОценок пока нет
- 2012 Aug IMG Poster 165760a SepsisДокумент1 страница2012 Aug IMG Poster 165760a SepsisTeng Huei LeeОценок пока нет
- EAU Pocket Guidelines Urological Infections 2019Документ22 страницыEAU Pocket Guidelines Urological Infections 2019felixОценок пока нет
- Drug Study GabrielaДокумент4 страницыDrug Study GabrielaNimrodОценок пока нет
- EAU Pocket Guidelines Urological - Infections 2012 PDFДокумент18 страницEAU Pocket Guidelines Urological - Infections 2012 PDFbrukner30Оценок пока нет
- Urinary Tract Infection (UTI) Definitions: PyelonephritisДокумент4 страницыUrinary Tract Infection (UTI) Definitions: PyelonephritisSanthosh KumarОценок пока нет
- UTI Algorithm-Inpatient RQHRДокумент1 страницаUTI Algorithm-Inpatient RQHRDe RadianОценок пока нет
- Prophylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofДокумент10 страницProphylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofElle RosalesОценок пока нет
- Pseudomonas Aeruginosa PfizerДокумент3 страницыPseudomonas Aeruginosa PfizerPutri Kania DewiОценок пока нет
- 8 Urinary Tract InfectionДокумент4 страницы8 Urinary Tract Infectionzainabd1964Оценок пока нет
- Escalation Guide For Gram-Negative Bacteremia StanfordДокумент3 страницыEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaОценок пока нет
- Drug Study: Adult: ChildДокумент4 страницыDrug Study: Adult: ChildKristian Karl Bautista Kiw-isОценок пока нет
- Anti - Infectives AgentsДокумент83 страницыAnti - Infectives AgentsRhien Yrah P. CabalongaОценок пока нет
- Bone and Joint Infections BNHFT 2010 PDFДокумент3 страницыBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriОценок пока нет
- Ringkasan Dosis Obat 7th RevisedДокумент38 страницRingkasan Dosis Obat 7th RevisedMuhammad IhsanuddinОценок пока нет
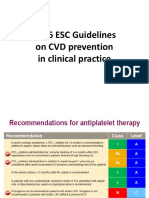
- 2016 ESC Guidelines On CVD Prevention in Clinical PracticeДокумент8 страниц2016 ESC Guidelines On CVD Prevention in Clinical PracticeMuhammad IhsanuddinОценок пока нет
- Referat Airway ManagementДокумент24 страницыReferat Airway ManagementVerarisnaОценок пока нет
- Ipa Belum Di TranslateДокумент5 страницIpa Belum Di TranslateMuhammad IhsanuddinОценок пока нет
- Mechanism Molecular SepsisДокумент4 страницыMechanism Molecular SepsisMuhammad IhsanuddinОценок пока нет
- Tourist Behaviour Unit I & IIДокумент83 страницыTourist Behaviour Unit I & IIRashmiranjanОценок пока нет
- Daftar Nama Dosen Pembimbing Periode 2020-1 PagiДокумент3 страницыDaftar Nama Dosen Pembimbing Periode 2020-1 PagiNufita Twandita DewiОценок пока нет
- Stochastic Frontier Analysis and DEAДокумент3 страницыStochastic Frontier Analysis and DEAHa M ZaОценок пока нет
- Moy Ya Lim Yao vs. Commissioner of ImmigrationG.R. No. L-21289 SCRA 292 DigestДокумент2 страницыMoy Ya Lim Yao vs. Commissioner of ImmigrationG.R. No. L-21289 SCRA 292 DigestKhen Tamdang100% (1)
- Unveiling The Factors Shaping Financial Choices Among Women in The Professional Sphere: An Analytical Framework Utilizing Structural Equation Modeling in Behavioral Finance.Документ17 страницUnveiling The Factors Shaping Financial Choices Among Women in The Professional Sphere: An Analytical Framework Utilizing Structural Equation Modeling in Behavioral Finance.International Journal of Innovative Science and Research TechnologyОценок пока нет
- Aperin TOS Entrepreneurship Grade12Документ2 страницыAperin TOS Entrepreneurship Grade12Arvin Austria AperinОценок пока нет
- Factors Affecting Young People Buying Decision On Green Products: A Case Study in Ho Chi Minh CityДокумент53 страницыFactors Affecting Young People Buying Decision On Green Products: A Case Study in Ho Chi Minh CityBăng BăngОценок пока нет
- The Making of R.A. 1425Документ3 страницыThe Making of R.A. 1425Reje CuaresmaОценок пока нет
- Management QuestionsДокумент5 страницManagement QuestionsAhmedAlhosaniОценок пока нет
- Kyrosoft Technologies: A User Guide & Manual OnДокумент20 страницKyrosoft Technologies: A User Guide & Manual OnjagsmcОценок пока нет
- College Thesis. - BSED - 2022Документ201 страницаCollege Thesis. - BSED - 2022Justin MirandoОценок пока нет
- Detailed Collection of All Synonyms From Cambridge IELTS BooksДокумент78 страницDetailed Collection of All Synonyms From Cambridge IELTS BooksAli Mehdi Maknojia92% (13)
- Team Building Breakout ScriptДокумент12 страницTeam Building Breakout ScriptMelanie PajaronОценок пока нет
- Interest GroupsДокумент25 страницInterest GroupsnikkivОценок пока нет
- English A SbaДокумент13 страницEnglish A Sbacarlton jackson50% (2)
- Unit23 SolutionsДокумент7 страницUnit23 SolutionsAbcОценок пока нет
- Cardiohelp System Brochure-En-Non Us JapanДокумент16 страницCardiohelp System Brochure-En-Non Us JapanAnar MaharramovОценок пока нет
- The Urantia Book (Public Domain)Документ1 806 страницThe Urantia Book (Public Domain)Lenny100% (13)
- Victor M Orozco 8860 SW 123 CT APT K310 Miami FL 33186Документ4 страницыVictor M Orozco 8860 SW 123 CT APT K310 Miami FL 33186Wa Riz LaiОценок пока нет
- Right On 1Документ2 страницыRight On 1Lingva Lingva BinestОценок пока нет
- Sets&StatisticsДокумент6 страницSets&StatisticsFarah AghaverdiyevaОценок пока нет
- Geo5 Fem Theoretical GuideДокумент113 страницGeo5 Fem Theoretical GuideAnonymous 87xpkIJ6CFОценок пока нет
- Meeresstille NotesДокумент5 страницMeeresstille NotesJayOngОценок пока нет
- 12th Bio Botany EM Important Questions English Medium PDF DownloadДокумент7 страниц12th Bio Botany EM Important Questions English Medium PDF DownloadPrase 1815Оценок пока нет
- Applying The Rossiter-Percy Grid To Online Advertising Planning - The Role of Product - Brand Type in Previsit IntentionsДокумент9 страницApplying The Rossiter-Percy Grid To Online Advertising Planning - The Role of Product - Brand Type in Previsit Intentionsa861108Оценок пока нет
- Covid FeversДокумент7 страницCovid FeversdbvidyaОценок пока нет
- Dictogloss Strategy and Listening Comprehension Performance of Secondary School StudentsДокумент12 страницDictogloss Strategy and Listening Comprehension Performance of Secondary School StudentsSilvi AlizaОценок пока нет
- Favoritism Bad Habbit of Some TeacherДокумент2 страницыFavoritism Bad Habbit of Some TeacherQasim TapsiОценок пока нет
- Cawis vs. Cerilles - G.R. No. 170207 - April 19, 2010Документ2 страницыCawis vs. Cerilles - G.R. No. 170207 - April 19, 2010Lordy Jessah AggabaoОценок пока нет
- Clase 1-Fisiopatología de La Artritis ReumatoideaДокумент45 страницClase 1-Fisiopatología de La Artritis ReumatoideaPercy Williams Mendoza EscobarОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (35)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeОт EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeРейтинг: 4.5 из 5 звезд4.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (5)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionОт EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionОценок пока нет
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsОт EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsРейтинг: 4.5 из 5 звезд4.5/5 (39)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (44)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОт EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОценок пока нет
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!От EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Рейтинг: 5 из 5 звезд5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (267)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedРейтинг: 4 из 5 звезд4/5 (61)