Вам также может понравиться
- The Consensus of Church Fathers On A Spherical EarthДокумент9 страницThe Consensus of Church Fathers On A Spherical EarthDan Constantin100% (3)
- 3D Volume Rendering and 3D Printing (Additive Manufacturing)Документ10 страниц3D Volume Rendering and 3D Printing (Additive Manufacturing)Natacha AlvesОценок пока нет
- Photopolymerjet 3D Printing Mai 2017Документ8 страницPhotopolymerjet 3D Printing Mai 2017Aatif KhanОценок пока нет
- Zaharin 2018 IOP Conf. Ser. - Mater. Sci. Eng. 328 012003 PDFДокумент8 страницZaharin 2018 IOP Conf. Ser. - Mater. Sci. Eng. 328 012003 PDFGet SazzidОценок пока нет
- Rapid Prototyping and Rapid Machining of Medical ImplantsДокумент8 страницRapid Prototyping and Rapid Machining of Medical ImplantsZaheer AhamedОценок пока нет
- Rapid Prototyping in DentistryДокумент13 страницRapid Prototyping in DentistryManjeevОценок пока нет
- 3d Printing 2Документ5 страниц3d Printing 2CherifОценок пока нет
- APRD - 2 (2) - 33-36 (B)Документ4 страницыAPRD - 2 (2) - 33-36 (B)Nur Syfa MufidhahОценок пока нет
- Manufacturing of Customized Implants For Orbital Fractures Using 3D PrintingДокумент6 страницManufacturing of Customized Implants For Orbital Fractures Using 3D PrintingManmadha CharyОценок пока нет
- 3D Printing - An Alternative of Conventional Crown Fabrication A Case ReportДокумент7 страниц3D Printing - An Alternative of Conventional Crown Fabrication A Case ReportBalavigneshwaran bt18ipf04Оценок пока нет
- 2019 High Quality Temporary Crowns and Bridge by StereolithographyДокумент7 страниц2019 High Quality Temporary Crowns and Bridge by StereolithographyAya Ibrahim YassinОценок пока нет
- Application of CAD/CAE & Rapid Prototyping Technology in Medical FieldДокумент5 страницApplication of CAD/CAE & Rapid Prototyping Technology in Medical FieldRizwanОценок пока нет
- Research ArticleДокумент9 страницResearch Articlemalpigi cisimciğiОценок пока нет
- Patient Specific Implants (Psi) in Maxillofacial Rehabilitation - A Systematic ReviewДокумент10 страницPatient Specific Implants (Psi) in Maxillofacial Rehabilitation - A Systematic ReviewIJAR JOURNALОценок пока нет
- Adaptability Evaluation of Metal-Ceramic Crowns ObДокумент12 страницAdaptability Evaluation of Metal-Ceramic Crowns ObVlad CheptanaruОценок пока нет
- Recent Advancements in Additive Manufacturing Technologies For Porous Material Applications.Документ23 страницыRecent Advancements in Additive Manufacturing Technologies For Porous Material Applications.Thành TânОценок пока нет
- Fratura de Resina Impressa e FresadaДокумент10 страницFratura de Resina Impressa e FresadaDanilo BianchiОценок пока нет
- Reverse Engineering in CAD Model Reconstruction of Customized Artificial JointДокумент5 страницReverse Engineering in CAD Model Reconstruction of Customized Artificial JointalexОценок пока нет
- Development of Porous Medical Implant Scaffolds ViaДокумент7 страницDevelopment of Porous Medical Implant Scaffolds ViajonkОценок пока нет
- Fit of Interim Crowns Fabricated Using Photopolymer-Jetting 3D PrintingДокумент9 страницFit of Interim Crowns Fabricated Using Photopolymer-Jetting 3D PrintingDina MahmoudNasrОценок пока нет
- 3D-Printing and Upper-Limb Prosthetic Sockets Promises and PitfallsДокумент9 страниц3D-Printing and Upper-Limb Prosthetic Sockets Promises and PitfallsGiancarlo PalaciosОценок пока нет
- Comparative Analysis of Fracture Resistance Between CAD - CAM Materials For Interim Fixed ProsthesisДокумент12 страницComparative Analysis of Fracture Resistance Between CAD - CAM Materials For Interim Fixed Prosthesisadriyeli22Оценок пока нет
- 3D Modeling, Custom Implants and Its FutureДокумент10 страниц3D Modeling, Custom Implants and Its FutureDrAhmed HamzaОценок пока нет
- Experimental and Finite Element Analysis of Titanium Based Medial Tibial Condyle Using Incremental Sheet Metal FormingДокумент7 страницExperimental and Finite Element Analysis of Titanium Based Medial Tibial Condyle Using Incremental Sheet Metal Forming戴翰明Оценок пока нет
- An Update On Applications of 3D Printing Technologies UsedДокумент8 страницAn Update On Applications of 3D Printing Technologies UsedAlex BurdeОценок пока нет
- Materials 12 01958Документ20 страницMaterials 12 01958Vishal SharmaОценок пока нет
- Prosthetic Sockets Fabrication Using Rapid Prototyping TechnologyДокумент7 страницProsthetic Sockets Fabrication Using Rapid Prototyping TechnologyHaider NeamaОценок пока нет
- Additive Manufacturing of Biomaterials For Bone TissueДокумент43 страницыAdditive Manufacturing of Biomaterials For Bone TissuedayseanedОценок пока нет
- Model Prediction of Defects in Sheet Metal Forming ProcessesДокумент12 страницModel Prediction of Defects in Sheet Metal Forming Processeschandra jemyОценок пока нет
- Assessment of The Internal Fit and Marginal Integrity of Interim Crowns Made by Different Manufacturing MethodsДокумент9 страницAssessment of The Internal Fit and Marginal Integrity of Interim Crowns Made by Different Manufacturing MethodsDina MahmoudNasrОценок пока нет
- 3D Printing Based On Imaging DataДокумент7 страниц3D Printing Based On Imaging DataWangi Pandan Sari0% (1)
- Jurnal 2 IngДокумент7 страницJurnal 2 IngSannia SalsabilaОценок пока нет
- Biomechanical Behavior of CADCAM Cobalt Chromium and Zirconia Full Arch FixedДокумент10 страницBiomechanical Behavior of CADCAM Cobalt Chromium and Zirconia Full Arch FixedGabriela CastroОценок пока нет
- Buap 6Документ11 страницBuap 6WawawaОценок пока нет
- 2017 Esthetic Rehabilitation of Anterior Teeth With Copy Milled RestorationsДокумент5 страниц2017 Esthetic Rehabilitation of Anterior Teeth With Copy Milled RestorationshadriaanaОценок пока нет
- Functional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedДокумент12 страницFunctional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedDoruk OrgunОценок пока нет
- Design, Printing Optimization, and Material Testing of A 3d-Printed Nasal Osteotomy Task TrainerДокумент6 страницDesign, Printing Optimization, and Material Testing of A 3d-Printed Nasal Osteotomy Task Trainerlabakoum badr-eddineОценок пока нет
- Adj 12748Документ8 страницAdj 12748Irfan HussainОценок пока нет
- Evolution of The Software and Hardware in CADCAM Systems Used in DentistryДокумент8 страницEvolution of The Software and Hardware in CADCAM Systems Used in DentistryMihociStefanОценок пока нет
- Stereolithographic Surgical Template: A Review: Abst TДокумент3 страницыStereolithographic Surgical Template: A Review: Abst Tairtifa1Оценок пока нет
- Custom Implant For The Mandible Using Rapidprototyping Assisted CastingДокумент5 страницCustom Implant For The Mandible Using Rapidprototyping Assisted Castingtushak mОценок пока нет
- PIIS0889540619306262Документ8 страницPIIS0889540619306262VALENTINA FERNANDA GALLARDO SANZANAОценок пока нет
- Research PaperДокумент10 страницResearch PaperMalik ahxanОценок пока нет
- Trueness of CADCAM Digitization With AДокумент14 страницTrueness of CADCAM Digitization With ABedah Mulut dan Maksilofasial 2023Оценок пока нет
- Pilot Study of The Wrist Orthosis Design ProcessДокумент7 страницPilot Study of The Wrist Orthosis Design ProcessRobert PetersonОценок пока нет
- Marginal and Internal Fit of 3D Printed ProvisionaДокумент8 страницMarginal and Internal Fit of 3D Printed Provisionamostafa fayezОценок пока нет
- International Journal of Dental Science and Innovative Research (IJDSIR)Документ10 страницInternational Journal of Dental Science and Innovative Research (IJDSIR)Danish NasirОценок пока нет
- PD - 1 - Literature ReviewДокумент19 страницPD - 1 - Literature ReviewMuhammad Wasif AnwarОценок пока нет
- Comparing The Accuracy Trueness and Precision of Models of Fixed Dental Prostheses Fabricated by Digital and Conventional Workflows 2019Документ6 страницComparing The Accuracy Trueness and Precision of Models of Fixed Dental Prostheses Fabricated by Digital and Conventional Workflows 2019ANDREA LOZANO CAMPOSОценок пока нет
- Acc Jurnal Pedo 1Документ10 страницAcc Jurnal Pedo 1Orintya DewiОценок пока нет
- Obturator DicomДокумент7 страницObturator DicomDina AbdelmoezОценок пока нет
- 3D Printing Turbine BladesДокумент21 страница3D Printing Turbine Blades19MECH052 SYED YOUNUSОценок пока нет
- Durão2019 Article OptimizingAdditiveManufacturinДокумент23 страницыDurão2019 Article OptimizingAdditiveManufacturinAlamОценок пока нет
- Cad Cam PDFДокумент7 страницCad Cam PDFOmanakuttan Kr100% (1)
- (IJCST-V8I2P2) : Veena N. JokhakarДокумент8 страниц(IJCST-V8I2P2) : Veena N. JokhakarEighthSenseGroupОценок пока нет
- 3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in BiomДокумент7 страниц3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in Biomrrm77Оценок пока нет
- Marginal Adaptation of CAD-CAM and Heat-Pressed Lithium Disilicate Crowns: A Systematic Review and Meta-AnalysisДокумент6 страницMarginal Adaptation of CAD-CAM and Heat-Pressed Lithium Disilicate Crowns: A Systematic Review and Meta-AnalysisMariana ThielОценок пока нет
- Classifications and Properties of Materials For Chairside (E.max CAD) and (Vitabloc Mark II)Документ15 страницClassifications and Properties of Materials For Chairside (E.max CAD) and (Vitabloc Mark II)Nguyễn Đức TuấnОценок пока нет
- Customised Design of A Patient Specific 3D Printed Whole Mandible ImplantДокумент8 страницCustomised Design of A Patient Specific 3D Printed Whole Mandible ImplantSAM IMОценок пока нет
- Scaffold Fabrication by Indirect Three-Dimensional Printing: Min Lee, James C.Y. Dunn, Benjamin M. WuДокумент9 страницScaffold Fabrication by Indirect Three-Dimensional Printing: Min Lee, James C.Y. Dunn, Benjamin M. WuCraciun AlexОценок пока нет
- Clinical Applications of Digital Dental TechnologyОт EverandClinical Applications of Digital Dental TechnologyRadi MasriОценок пока нет
- Mensuration II (Important Results)Документ8 страницMensuration II (Important Results)Kshitij KumarОценок пока нет
- CH 01 More QuestionsДокумент16 страницCH 01 More Questionswoboc79249Оценок пока нет
- 2018 YJC H2 Prelim P1 + SolutionДокумент19 страниц2018 YJC H2 Prelim P1 + Solutiontoh tim lamОценок пока нет
- Cbjemapl09 PDFДокумент8 страницCbjemapl09 PDFsngayu6522Оценок пока нет
- 8.isometric Projections and Isometric View or DrawingДокумент39 страниц8.isometric Projections and Isometric View or DrawingMahek JariwalaОценок пока нет
- 17 - Sound WavesДокумент26 страниц17 - Sound WavesresОценок пока нет
- Potential - Fields ExercisesДокумент2 страницыPotential - Fields ExercisesMohamed KessyОценок пока нет
- Elementary Mathematical Astronomy, Barlow & BryanДокумент460 страницElementary Mathematical Astronomy, Barlow & Bryanandresmejia68100% (1)
- 5 Unsol OIQ Math 10thДокумент8 страниц5 Unsol OIQ Math 10thOmshree PanigrahiОценок пока нет
- Department of Civil Engineering: I. Problem SolvingДокумент2 страницыDepartment of Civil Engineering: I. Problem SolvingEnrique NebridaОценок пока нет
- ASME Pressure VesselsДокумент41 страницаASME Pressure VesselsJawed Akhter100% (1)
- Class 12 National Genius Search Examination: Advanced: Test CodeДокумент8 страницClass 12 National Genius Search Examination: Advanced: Test CodePPОценок пока нет
- June 2018 4h - UnlockedДокумент24 страницыJune 2018 4h - UnlockedahmedОценок пока нет
- Pressure Vessel Weight DeterminationДокумент33 страницыPressure Vessel Weight DeterminationToni100% (5)
- 12 Seater Business Jet Design: A Conceptual ApproachДокумент24 страницы12 Seater Business Jet Design: A Conceptual ApproachPrashanth Natarajan IyerОценок пока нет
- 2020 4U - Parramatta Marist - Trial Paper (With Solutions)Документ28 страниц2020 4U - Parramatta Marist - Trial Paper (With Solutions)Reacher ElliotОценок пока нет
- Igcse MB-PM Syllabus BreakdownДокумент4 страницыIgcse MB-PM Syllabus BreakdownabrarjayОценок пока нет
- Physics Lesson Note SS2 3rd Term, 2023 - 1Документ56 страницPhysics Lesson Note SS2 3rd Term, 2023 - 1aloooab9Оценок пока нет
- Mathematics 3Документ16 страницMathematics 3mccolisterbusiso36Оценок пока нет
- Solid AngleДокумент9 страницSolid AngleDimitrios Christos SarvanisОценок пока нет
- Programming C Mid TermДокумент4 страницыProgramming C Mid TermlindaОценок пока нет
- Geometry Common CoreДокумент4 страницыGeometry Common Coreapi-153767556Оценок пока нет
- Computer Graphics Prof. Sukhendu Das Dept. of Computer Science and Engineering Indian Institute of Technology, Madras Lecture-23 Solid ModellingДокумент20 страницComputer Graphics Prof. Sukhendu Das Dept. of Computer Science and Engineering Indian Institute of Technology, Madras Lecture-23 Solid ModellingBalaji VfxОценок пока нет
- Determination of The Molecular Weight of A Polymer Via Oswald ViscometryДокумент8 страницDetermination of The Molecular Weight of A Polymer Via Oswald ViscometryfruitfuckОценок пока нет
- Review 2Документ4 страницыReview 2Jonas CayananОценок пока нет
- 93 Info View Factors Catalog J R HowellДокумент72 страницы93 Info View Factors Catalog J R HowellPiyush AgarwalОценок пока нет
- Autodyn SPH User Manual & TutorialДокумент73 страницыAutodyn SPH User Manual & TutorialmindertОценок пока нет
- Test-Paper-6: Physics Time: 1hr Date: 23-12-2020 Multi-Choice Single Correct (+3,0,-1)Документ12 страницTest-Paper-6: Physics Time: 1hr Date: 23-12-2020 Multi-Choice Single Correct (+3,0,-1)NdjskaОценок пока нет
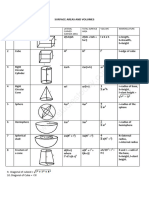
- Surface Area and Volume Assignment 13Документ4 страницыSurface Area and Volume Assignment 13emberlyn.sternsОценок пока нет