Вам также может понравиться
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionОт EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionОценок пока нет
- Aota PDFДокумент2 страницыAota PDFJuliana MassariolliОценок пока нет
- StrokeДокумент5 страницStrokeapi-261670650Оценок пока нет
- Occupational AdaptationДокумент5 страницOccupational AdaptationVASH12345100% (1)
- Position Paper OT For People With LDДокумент10 страницPosition Paper OT For People With LDLytiana WilliamsОценок пока нет
- Occupational Therapy Examination Review Guide 4th Edition Ebook PDFДокумент57 страницOccupational Therapy Examination Review Guide 4th Edition Ebook PDFrobert.campbell485Оценок пока нет
- Occupational Therapy and Mental Health 1Документ18 страницOccupational Therapy and Mental Health 1Roman -Оценок пока нет
- Ebp PaperДокумент16 страницEbp Paperapi-583545759Оценок пока нет
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidДокумент20 страницOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818Оценок пока нет
- Aus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingДокумент11 страницAus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingMelissa CroukampОценок пока нет
- Ota Group ProtocolДокумент26 страницOta Group Protocolapi-318685839Оценок пока нет
- Client-Centered AssessmentДокумент4 страницыClient-Centered AssessmentHon “Issac” KinHoОценок пока нет
- Occupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and TreatmentДокумент13 страницOccupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and Treatmentapi-234120429Оценок пока нет
- Integration of Medication Management Into Occupational Therapy PracticeДокумент7 страницIntegration of Medication Management Into Occupational Therapy PracticeManuel PérezОценок пока нет
- Effectiveness of Occupation-Based Interventions To Improve Areas of Occupation and Social Participation After StrokeДокумент11 страницEffectiveness of Occupation-Based Interventions To Improve Areas of Occupation and Social Participation After StrokeSandra BarbazanОценок пока нет
- Model of Human Occupation Parts 1-4Документ36 страницModel of Human Occupation Parts 1-4Alice GiffordОценок пока нет
- Occupation Analysis in PracticeОт EverandOccupation Analysis in PracticeLynette MackenzieОценок пока нет
- Cimt and NDT Proposal-2 AltДокумент10 страницCimt and NDT Proposal-2 Altapi-487111274Оценок пока нет
- Critique Form For Critical Appraisal Students Name: - Date: - DirectionsДокумент6 страницCritique Form For Critical Appraisal Students Name: - Date: - DirectionsEsther BrooksОценок пока нет
- Placement HandbookДокумент551 страницаPlacement HandbookAdonis GaleosОценок пока нет
- Occupational Therapy in Oncology and Palliative CareДокумент10 страницOccupational Therapy in Oncology and Palliative CareSenthil KumarОценок пока нет
- Occupational JusticeДокумент4 страницыOccupational JusticeHardeep Singh BaliОценок пока нет
- Occupation in Occupational Therapy PDFДокумент26 страницOccupation in Occupational Therapy PDFa_tobarОценок пока нет
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceДокумент53 страницыStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiОценок пока нет
- Meaningful OccupationДокумент13 страницMeaningful OccupationSyafiq Azzmi100% (1)
- Program ProposalДокумент17 страницProgram Proposalapi-582621575Оценок пока нет
- Gilfoyle 1984 Slagle LectureДокумент14 страницGilfoyle 1984 Slagle LectureDebbieОценок пока нет
- Cognition, Cognitive Rehabilitation, and Occupational PerformanceДокумент23 страницыCognition, Cognitive Rehabilitation, and Occupational PerformanceMaria AiramОценок пока нет
- OTB 502 Syllabus 2019Документ22 страницыOTB 502 Syllabus 2019Gehan BotorsОценок пока нет
- OT8 - Thumb Immobilization SplintДокумент4 страницыOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
- Community Mental HealthДокумент2 страницыCommunity Mental HealthGhea Mae Jukebox VillasОценок пока нет
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Документ54 страницы2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18Оценок пока нет
- AДокумент7 страницARaphael AguiarОценок пока нет
- 2 Introduction To TheoryДокумент14 страниц2 Introduction To TheoryNurul Izzah Wahidul AzamОценок пока нет
- CC StrokeДокумент13 страницCC Strokeapi-436090845100% (1)
- Hazley Jarrett Jordan-Final Cimt Systematic Review AltДокумент14 страницHazley Jarrett Jordan-Final Cimt Systematic Review Altapi-518986604Оценок пока нет
- Opening A Private Practice in Occupational Therapy: Earn .1 Aota CeuДокумент9 страницOpening A Private Practice in Occupational Therapy: Earn .1 Aota CeuRey John MonjeОценок пока нет
- Soap NoteДокумент2 страницыSoap Noteapi-285542134Оценок пока нет
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyДокумент16 страницActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraОценок пока нет
- OT Models PratciceДокумент30 страницOT Models PratciceWalaa Eldesoukey100% (1)
- Instrumental Activities Daily Living: Try ThisДокумент11 страницInstrumental Activities Daily Living: Try ThisbalryoОценок пока нет
- OT and Eating DysfunctionДокумент1 страницаOT and Eating DysfunctionMCris EsSemОценок пока нет
- Instructor's Manual: Catherine Meriano, JD, MHS, OTR/LДокумент10 страницInstructor's Manual: Catherine Meriano, JD, MHS, OTR/LDaNelle McPhaddenОценок пока нет
- Occupational Therapy ProcessДокумент3 страницыOccupational Therapy Processapi-339841373100% (1)
- Rabideau Kitchen Eval AjotДокумент8 страницRabideau Kitchen Eval Ajotapi-291380671Оценок пока нет
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeДокумент55 страницThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (2)
- Understanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementДокумент11 страницUnderstanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementAlejandroAndrésAlvarezContrerasОценок пока нет
- Key Responsibilities:: Occupational Therapist Job Description V-Jan/2020Документ4 страницыKey Responsibilities:: Occupational Therapist Job Description V-Jan/2020MD Luthfy LubisОценок пока нет
- OccupationalTherapy - Williams SyndromeДокумент4 страницыOccupationalTherapy - Williams SyndromejuanmorerosfОценок пока нет
- Initial TemplateДокумент8 страницInitial TemplateZuj PayОценок пока нет
- Working As An Occupational Therapist in Another Country 2015Документ101 страницаWorking As An Occupational Therapist in Another Country 2015RLedgerdОценок пока нет
- Vergara, J. - T.O. in The Neonatal Intensive Care UnitДокумент11 страницVergara, J. - T.O. in The Neonatal Intensive Care UnitFedora Margarita Santander CeronОценок пока нет
- Artifact 5 Soap NoteДокумент3 страницыArtifact 5 Soap Noteapi-517998988Оценок пока нет
- The+Model+of+Creative+AbilityДокумент22 страницыThe+Model+of+Creative+AbilitysandeepОценок пока нет
- Guidelines For Documentation of Occupational Therapy PDFДокумент7 страницGuidelines For Documentation of Occupational Therapy PDFMaria AiramОценок пока нет
- The Occupational Brain A Theory of Human NatureДокумент6 страницThe Occupational Brain A Theory of Human NatureJoaquin OlivaresОценок пока нет
- History of OT Infographic TimelineДокумент1 страницаHistory of OT Infographic TimelineAddissa MarieОценок пока нет
- OT Code of Ethics 2015Документ8 страницOT Code of Ethics 2015Ays OlarteОценок пока нет
- Part 2: Social Skills Training: RatingДокумент3 страницыPart 2: Social Skills Training: RatingGina GucioОценок пока нет
- AOTA Occupational Profile Template PDFДокумент2 страницыAOTA Occupational Profile Template PDFCrys Paola Alvarez GonzalezОценок пока нет
- GRADES 1 To 12 Daily Lesson Log Friday Thursday Wednesday Tuesday MondayДокумент2 страницыGRADES 1 To 12 Daily Lesson Log Friday Thursday Wednesday Tuesday MondaychoyОценок пока нет
- Lesson 2 - La Casa (The House) : This Week's New WordsДокумент10 страницLesson 2 - La Casa (The House) : This Week's New WordsSylvia Ana Maria TeodorescuОценок пока нет
- Goof Proof GrammarДокумент140 страницGoof Proof GrammarJosué Maximin ANDÉОценок пока нет
- Analytical Philosophy in Comparative Perspective PDFДокумент407 страницAnalytical Philosophy in Comparative Perspective PDFCecco AngiolieriОценок пока нет
- IELTS Reading Passage 3 - Endangered LanguageДокумент2 страницыIELTS Reading Passage 3 - Endangered LanguagePradeep PaudelОценок пока нет
- Behavioral Aspects of Solid Waste Management A Systematic ReviewДокумент36 страницBehavioral Aspects of Solid Waste Management A Systematic ReviewAbeer El ShahawyОценок пока нет
- MODUL GRAMMAR INFINITIVE PHRASE GENERAL FORM and PERFECT FORM of INFINITIVE PHRASEДокумент6 страницMODUL GRAMMAR INFINITIVE PHRASE GENERAL FORM and PERFECT FORM of INFINITIVE PHRASEAmelie's Story100% (1)
- The Basics of Troubleshooting Engine Room MachineryДокумент5 страницThe Basics of Troubleshooting Engine Room MachineryJhay Sustiguer67% (3)
- Impact: Philosophical Perspectives On Education PolicyДокумент40 страницImpact: Philosophical Perspectives On Education Policyjoseph s. butawanОценок пока нет
- Understanding The SelfДокумент3 страницыUnderstanding The SelfMica Krizel Javero MercadoОценок пока нет
- Giving Tree Lesson PlanДокумент2 страницыGiving Tree Lesson Planapi-372294211Оценок пока нет
- Second Quarter: Positive and Negative Messages Conveyed in AДокумент3 страницыSecond Quarter: Positive and Negative Messages Conveyed in AMACAINAG, AngelicaОценок пока нет
- Presentation of PolitenessДокумент13 страницPresentation of PolitenessNashwa RashedОценок пока нет
- Possessive Adjectives and Pronouns Cuarto PeriodoДокумент5 страницPossessive Adjectives and Pronouns Cuarto PeriodowilfredoОценок пока нет
- Information Retrieval and Web SearchДокумент29 страницInformation Retrieval and Web SearchaymancvaОценок пока нет
- Teaching English Word-Formation Processes in EFL ContextДокумент28 страницTeaching English Word-Formation Processes in EFL ContextMengiОценок пока нет
- Historical Journal Entry Rubricworld HistoryДокумент2 страницыHistorical Journal Entry Rubricworld Historyapi-241347803Оценок пока нет
- LOT 2: The Language of Thought RevisitedДокумент6 страницLOT 2: The Language of Thought Revisitedالملاك الابيضОценок пока нет
- Teaching PronunciationДокумент18 страницTeaching PronunciationYanling Li100% (1)
- Global Test 4 1st SemesterДокумент2 страницыGlobal Test 4 1st Semesterr saberОценок пока нет
- Summer Project Curriculum Final DraftДокумент98 страницSummer Project Curriculum Final DraftSyahari100% (1)
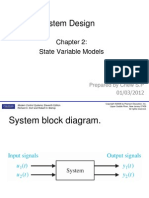
- Chapter 2 - State Space RepresentationДокумент32 страницыChapter 2 - State Space RepresentationShah EmerulОценок пока нет
- Negotiation Skills ReportДокумент13 страницNegotiation Skills ReportDEWASHISH RAIОценок пока нет
- Communication - I. Communication Skills: Approaches To Learning - (Atl Skills)Документ4 страницыCommunication - I. Communication Skills: Approaches To Learning - (Atl Skills)PoloОценок пока нет
- Factors Affecting Job Satisfaction of Employees in A Public InstitutionДокумент145 страницFactors Affecting Job Satisfaction of Employees in A Public InstitutionJunedyn TurdilОценок пока нет
- CLIL & TASK-BASED APPROACH (Ventajas y Desventajas)Документ4 страницыCLIL & TASK-BASED APPROACH (Ventajas y Desventajas)Khristian DanielОценок пока нет
- Models of Communication: Miss Riza O. VillanuevaДокумент53 страницыModels of Communication: Miss Riza O. VillanuevaBea Dacillo BautistaОценок пока нет
- Instructional Design D. LemonДокумент57 страницInstructional Design D. LemonWilliam BuquiaОценок пока нет
- New Curriculum Formative Assessment NCDCДокумент26 страницNew Curriculum Formative Assessment NCDCRobert Kityo ProОценок пока нет
- Beyond Structural Listening PDFДокумент346 страницBeyond Structural Listening PDFАлександр Земцов100% (1)