Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Dell W2306C LCD Monitor Service ManualДокумент104 страницыDell W2306C LCD Monitor Service ManualIsrael B ChavezОценок пока нет
- Time Value of Money LectureДокумент54 страницыTime Value of Money LectureRanin, Manilac Melissa SОценок пока нет
- Accuity: High Speed Automated 2D & 3D Optical Gauging Single Click Setup and InspectionДокумент4 страницыAccuity: High Speed Automated 2D & 3D Optical Gauging Single Click Setup and InspectionAPPLEОценок пока нет
- ASCE Snow Loads On Solar-Paneled RoofsДокумент61 страницаASCE Snow Loads On Solar-Paneled RoofsBen100% (1)
- Motor CAT C13 AcertДокумент3 страницыMotor CAT C13 AcertJosé Gonzalez100% (4)
- Accsap 10 VHDДокумент94 страницыAccsap 10 VHDMuhammad Javed Gaba100% (2)
- Clinical Case StudyДокумент20 страницClinical Case Studyapi-252004748Оценок пока нет
- Calibration of Force ReductionДокумент36 страницCalibration of Force Reductionvincenzo_12613735Оценок пока нет
- YellowstoneДокумент1 страницаYellowstoneOana GalbenuОценок пока нет
- Chapter 10 - The Mature ErythrocyteДокумент55 страницChapter 10 - The Mature ErythrocyteSultan AlexandruОценок пока нет
- Comparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanДокумент4 страницыComparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanMasood HassanОценок пока нет
- Active Faults in MalaysiaДокумент52 страницыActive Faults in MalaysiaHazim HaОценок пока нет
- Tsel Manual ThermoselДокумент25 страницTsel Manual ThermoselPedro AlvelaisОценок пока нет
- Uji Efektivitas Mikroba Rumpun BambuДокумент7 страницUji Efektivitas Mikroba Rumpun BambuUse Real ProjectОценок пока нет
- Milviz F-15e Poh V 2Документ499 страницMilviz F-15e Poh V 2Jose Ramon Martinez GutierrezОценок пока нет
- Angewandte: ChemieДокумент13 страницAngewandte: ChemiemilicaОценок пока нет
- The Wilson Quarterly: The World's New Numbers by Martin WalkerДокумент13 страницThe Wilson Quarterly: The World's New Numbers by Martin WalkerDavid WeekОценок пока нет
- Hazard Assessment For PPE - XX-DRAFTДокумент4 страницыHazard Assessment For PPE - XX-DRAFTWayne VanderhoofОценок пока нет
- Reloved - October 2015Документ116 страницReloved - October 2015Barron Fields67% (3)
- Greater Occipital Nerve Block: Pain ManagementДокумент3 страницыGreater Occipital Nerve Block: Pain Managementkillingeyes177Оценок пока нет
- BECO UACE Chem2Документ6 страницBECO UACE Chem2EMMANUEL BIRUNGIОценок пока нет
- Iron Ore ProcessДокумент52 страницыIron Ore Processjafary448067% (3)
- Antoine Constants PDFДокумент3 страницыAntoine Constants PDFsofiaОценок пока нет
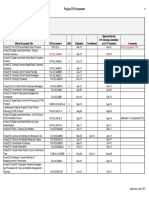
- Approved Project 25 StandardsДокумент5 страницApproved Project 25 StandardsepidavriosОценок пока нет
- 20160323014547-16MnCr5 - 16MnCrS5Документ1 страница20160323014547-16MnCr5 - 16MnCrS5Chaitanya DattaОценок пока нет
- Salapare Et Al 2015 ZambalesДокумент12 страницSalapare Et Al 2015 ZambalesTiqfar AhmadjayadiОценок пока нет
- Generalized Anxiety DisorderДокумент24 страницыGeneralized Anxiety DisorderEula Angelica OcoОценок пока нет