Вам также может понравиться
- Today! 2 Activity Book AKДокумент10 страницToday! 2 Activity Book AKMark Arenz Corixmir80% (5)
- Nursing Practice Skills: Adult Intensive Care Unit PatientsДокумент10 страницNursing Practice Skills: Adult Intensive Care Unit PatientsMona Doria67% (3)
- Art 06Документ6 страницArt 06He AfОценок пока нет
- Paula FM, Gryschek RCB, Chieffi PP - 2019 - Diagnosis of Strongyloides StercoralisДокумент3 страницыPaula FM, Gryschek RCB, Chieffi PP - 2019 - Diagnosis of Strongyloides StercoralisayresrenatoОценок пока нет
- 1 s2.0 S2341287923000078 MainДокумент7 страниц1 s2.0 S2341287923000078 MainyolandaОценок пока нет
- LGBS Lancet SeminarДокумент11 страницLGBS Lancet SeminarrSОценок пока нет
- Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityДокумент11 страницPrevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityAna LemesОценок пока нет
- MAKALAH Keputusasan-1Документ7 страницMAKALAH Keputusasan-1ARINAОценок пока нет
- 2016 Article 645Документ10 страниц2016 Article 645Betharia TriayuОценок пока нет
- Arch Dis Child 1998 Ladhani 85 8Документ5 страницArch Dis Child 1998 Ladhani 85 8Dian Ayu Permata SandiОценок пока нет
- Answers To Continuing Medical Education QuestionsДокумент2 страницыAnswers To Continuing Medical Education QuestionsKhalid AbdullahОценок пока нет
- DKM 037Документ7 страницDKM 037AyestinОценок пока нет
- 1 s2.0 S141386702300003X MainДокумент3 страницы1 s2.0 S141386702300003X MainLeonardo BarrosoОценок пока нет
- Article 1Документ6 страницArticle 1AMILA SYAZLINAОценок пока нет
- Amebiasis. Aspectos Clínicos, Terapéuticos y de Diagnóstico PDFДокумент7 страницAmebiasis. Aspectos Clínicos, Terapéuticos y de Diagnóstico PDFDina EuniseОценок пока нет
- Bacterial Control of Host Gene ExpressioДокумент14 страницBacterial Control of Host Gene ExpressioJose Leonel Fajardo RapaloОценок пока нет
- Prevención de La Neumonía Adquirida en La Comunidad: Prrevention of Community-Acquired Pneumonia in AdultsДокумент8 страницPrevención de La Neumonía Adquirida en La Comunidad: Prrevention of Community-Acquired Pneumonia in AdultsEileen Torres CerdaОценок пока нет
- Detection of Typhoid CarriersДокумент6 страницDetection of Typhoid CarriersClarestaОценок пока нет
- 2015 The Comparison Between Microhematocrit and Automated Methods For Hematocrit DeterminationДокумент10 страниц2015 The Comparison Between Microhematocrit and Automated Methods For Hematocrit DeterminationAgri Febria SariОценок пока нет
- Utility of Serological Tests in The Era of Molecular Testing For Diagnosis of Human Brucellosis in Endemic Area With Limited ResourcesДокумент4 страницыUtility of Serological Tests in The Era of Molecular Testing For Diagnosis of Human Brucellosis in Endemic Area With Limited ResourcesMiguel Pinedo TrujilloОценок пока нет
- Understanding Resistance vs. Susceptibility in Visceral Leishmaniasis Using Mouse Models of Leishmania Infantum InfectionДокумент14 страницUnderstanding Resistance vs. Susceptibility in Visceral Leishmaniasis Using Mouse Models of Leishmania Infantum InfectionAhmed RubaieОценок пока нет
- 9-Diagnosis of Malaria InfectionДокумент27 страниц9-Diagnosis of Malaria InfectionMazterMaztermaztermazter MaztermaztermazterYandeОценок пока нет
- Meningitis Bacteriana Aguda en El AdultoДокумент12 страницMeningitis Bacteriana Aguda en El AdultoJulian AlbarracínОценок пока нет
- Mourtzoukou Et Al-2008-British Journal of SurgeryДокумент8 страницMourtzoukou Et Al-2008-British Journal of SurgeryTony AdeosunОценок пока нет
- Different Diagnostic Procedure of Typhoid Fever AДокумент8 страницDifferent Diagnostic Procedure of Typhoid Fever AdjebrutОценок пока нет
- Amebiasis: Aspectos Clínicos, Terapéuticos y de Diagnóstico de La InfecciónДокумент8 страницAmebiasis: Aspectos Clínicos, Terapéuticos y de Diagnóstico de La Infección2022110046 HERNANDO JOSE DIAZ GONZALEZ ESTUDIANTE ACTIVOОценок пока нет
- B D GlukanДокумент6 страницB D GlukanAnja LjiljaОценок пока нет
- Articulo 7 Mig OkДокумент11 страницArticulo 7 Mig Okoscarbio20090% (1)
- Jurnal Viro AccДокумент6 страницJurnal Viro AccMelisa FransiskaОценок пока нет
- PCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative PathogensДокумент7 страницPCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative Pathogensfaraz.mirza1Оценок пока нет
- 3 Saritanayak EtalДокумент7 страниц3 Saritanayak EtaleditorijmrhsОценок пока нет
- Dxto de Infecciones en El SNCДокумент17 страницDxto de Infecciones en El SNCcarlos ballestasОценок пока нет
- Typhoid Fever: Diagnosis Blood and Bone Marrow Culture Faecal and Urine CulturesДокумент3 страницыTyphoid Fever: Diagnosis Blood and Bone Marrow Culture Faecal and Urine CulturesDila LarasatiОценок пока нет
- Clinical Value of Serology For The Diagnosis of Strongyloidiasis in Travelers and Migrants - A 4-Year Retrospective Study Using The Bordier IVD Strongyloides Ratti ELISA AssayДокумент10 страницClinical Value of Serology For The Diagnosis of Strongyloidiasis in Travelers and Migrants - A 4-Year Retrospective Study Using The Bordier IVD Strongyloides Ratti ELISA Assaygwyneth.green.512Оценок пока нет
- Susceptibility and Molecular Characterization of Species From Patients With VulvovaginitisДокумент8 страницSusceptibility and Molecular Characterization of Species From Patients With VulvovaginitisiisisiisОценок пока нет
- Nonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovanniДокумент14 страницNonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovannikaeranОценок пока нет
- Persistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneДокумент7 страницPersistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneMark ReinhardtОценок пока нет
- ORATORIO Ocrelizumab EMPPДокумент12 страницORATORIO Ocrelizumab EMPPalmarazneurologiaОценок пока нет
- 209 Full PDFДокумент8 страниц209 Full PDFAngga PratamaОценок пока нет
- Pathophysiology of Campylobacter Jejuni Infections of Humans 1999 Microbes and InfectionДокумент11 страницPathophysiology of Campylobacter Jejuni Infections of Humans 1999 Microbes and InfectionFrancisco GonzálezОценок пока нет
- Serologi 2Документ13 страницSerologi 2Syifa SariОценок пока нет
- Topic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"Документ26 страницTopic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"deekshit dcОценок пока нет
- Chou Dhuri 2012Документ10 страницChou Dhuri 2012yakoub bensaadaОценок пока нет
- 1 s2.0 S0168827804905533 MainДокумент1 страница1 s2.0 S0168827804905533 Maindjafer maryaОценок пока нет
- Immunity To Hep CДокумент11 страницImmunity To Hep CChelsey WilsonОценок пока нет
- ArticleДокумент16 страницArticleTunde OdetoyinОценок пока нет
- Art 3A10.1007 2Fs00405 009 0988 6Документ6 страницArt 3A10.1007 2Fs00405 009 0988 6mfhfhfОценок пока нет
- Infectious Diseases: Hepatitis C Virus Core Antigen Assay: Can We Think Beyond Convention in Resource Limited Settings?Документ6 страницInfectious Diseases: Hepatitis C Virus Core Antigen Assay: Can We Think Beyond Convention in Resource Limited Settings?Lee-Ya AchmadОценок пока нет
- Stroke in Two Children With Mycoplasma Pneumoniae Infection A Causal or Casual RelationshipДокумент15 страницStroke in Two Children With Mycoplasma Pneumoniae Infection A Causal or Casual Relationshipwawa chenОценок пока нет
- Weil-Felix Test in Diagnosis of ScrubДокумент3 страницыWeil-Felix Test in Diagnosis of ScrubvyasakandarpОценок пока нет
- Genlabs 2nlab GSFP p8f5 ReviewДокумент13 страницGenlabs 2nlab GSFP p8f5 ReviewElisabethОценок пока нет
- A Systematic Review of Bacteremias in Cellulitis and ErysipelasДокумент8 страницA Systematic Review of Bacteremias in Cellulitis and Erysipelasjenifer paathОценок пока нет
- Next Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostДокумент4 страницыNext Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostAthenaeum Scientific PublishersОценок пока нет
- CID Evaluation of Laboratory Methods For Diagnosis of VaricellaДокумент10 страницCID Evaluation of Laboratory Methods For Diagnosis of VaricellaK3 KoordinatorОценок пока нет
- Etiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyДокумент9 страницEtiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyNurul Dwi LestariОценок пока нет
- 4 KNДокумент25 страниц4 KNMohammad Yusuf AlamudiОценок пока нет
- 96443superior Biosensors For Detection of Pathogens Related To Livestock and PoultryДокумент3 страницы96443superior Biosensors For Detection of Pathogens Related To Livestock and PoultryietureoohiОценок пока нет
- Adaptation To The Host and Persistence: Role of Loss of Capsular Polysaccharide ExpressionДокумент10 страницAdaptation To The Host and Persistence: Role of Loss of Capsular Polysaccharide ExpressionIslam ZhyanmaОценок пока нет
- Meningite Aguda Bacteriana Rev Lancet 2016Документ12 страницMeningite Aguda Bacteriana Rev Lancet 2016elsonverdadeОценок пока нет
- Procedure: Monitoring, 3Документ2 страницыProcedure: Monitoring, 3Sebastian LopezОценок пока нет
- Culture Negative SepsisДокумент5 страницCulture Negative SepsismalvindersahiОценок пока нет
- Viral Hepatitis: Acute HepatitisОт EverandViral Hepatitis: Acute HepatitisResat OzarasОценок пока нет
- Content ServerДокумент9 страницContent ServerRahma RafinaОценок пока нет
- Ecg in Physical EvaluationsДокумент5 страницEcg in Physical EvaluationsandriopaОценок пока нет
- I Believe I'll Dust My BroomДокумент10 страницI Believe I'll Dust My BroomandriopaОценок пока нет
- Content ServerДокумент9 страницContent ServerRahma RafinaОценок пока нет
- Cooney Et Al-2013-Cochrane Database of Systematic ReviewsДокумент125 страницCooney Et Al-2013-Cochrane Database of Systematic ReviewsandriopaОценок пока нет
- Acute Coronary Syndrome PDFДокумент8 страницAcute Coronary Syndrome PDFVedranaJovanovicОценок пока нет
- Antibiotics NhsДокумент107 страницAntibiotics NhsandriopaОценок пока нет
- A 65-Year-Old Man Came To The Emergency Department Via Ambulance - Relatives Accompanied The Patient and Described A 1-Day History of FeverДокумент43 страницыA 65-Year-Old Man Came To The Emergency Department Via Ambulance - Relatives Accompanied The Patient and Described A 1-Day History of FeverandriopaОценок пока нет
- 2003 - A Macro Directive Mechanism That Facilitates Automatic Updating and Processing of The Contents of Electronic Healthcare Records An Extension To TheДокумент22 страницы2003 - A Macro Directive Mechanism That Facilitates Automatic Updating and Processing of The Contents of Electronic Healthcare Records An Extension To TheandriopaОценок пока нет
- Malaria in Greece 2012Документ10 страницMalaria in Greece 2012andriopaОценок пока нет
- Gulhane StadyДокумент6 страницGulhane StadyandriopaОценок пока нет
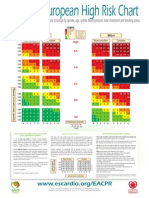
- 10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusДокумент2 страницы10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusCotovici Catana AlinaОценок пока нет
- Malaria in Greece 2012Документ10 страницMalaria in Greece 2012andriopaОценок пока нет
- Attack Rate of Influenza Cross Sectional DataДокумент11 страницAttack Rate of Influenza Cross Sectional DataandriopaОценок пока нет
- EndoДокумент7 страницEndoandriopaОценок пока нет
- HB Blood Component Transfusion Mod1 Rev01Документ30 страницHB Blood Component Transfusion Mod1 Rev01andriopaОценок пока нет
- Cancer MortalityДокумент5 страницCancer MortalityandriopaОценок пока нет
- 2013 Malaria in LakoniaДокумент6 страниц2013 Malaria in LakoniaandriopaОценок пока нет
- BLS HP 2015 V6.0 Student ManualДокумент33 страницыBLS HP 2015 V6.0 Student ManualandriopaОценок пока нет
- Evidence Based Decision MakingДокумент28 страницEvidence Based Decision MakingandriopaОценок пока нет
- The Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?Документ2 страницыThe Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?andriopaОценок пока нет
- 2006 Influence of ParacelsusДокумент6 страниц2006 Influence of ParacelsusandriopaОценок пока нет
- Nejms 1812.1Документ114 страницNejms 1812.1andriopaОценок пока нет
- Case Fatality Ratio PDFДокумент8 страницCase Fatality Ratio PDFandriopaОценок пока нет
- Case Fatality Ratio PDFДокумент8 страницCase Fatality Ratio PDFandriopaОценок пока нет
- HorticultureДокумент12 страницHorticultureवरुण राठीОценок пока нет
- BTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationДокумент11 страницBTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationEmaFediFeniОценок пока нет
- BKC 80Документ2 страницыBKC 80jawaidchemicalsОценок пока нет
- DP16B Bench Drill PressДокумент20 страницDP16B Bench Drill Pressalfri7370% (1)
- Whirlpool Adg 789Документ22 страницыWhirlpool Adg 789Laurentiu GramaОценок пока нет
- bNSG9000 Datasheet 2Документ3 страницыbNSG9000 Datasheet 2RobertОценок пока нет
- 365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusДокумент10 страниц365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusER Aditya DasОценок пока нет
- kAmAxI Muka Panchashati EngДокумент25 страницkAmAxI Muka Panchashati EngSrinathvr100% (1)
- Transient Stability of A Multi Machine Power System: Devender Kumar, Balwinder Singh SurjanДокумент4 страницыTransient Stability of A Multi Machine Power System: Devender Kumar, Balwinder Singh SurjanVerruumm AmineОценок пока нет
- Buku Murid Bahasa Inggris - Student's Book My Next Word For Elementary School Unit 10 - Fase BДокумент8 страницBuku Murid Bahasa Inggris - Student's Book My Next Word For Elementary School Unit 10 - Fase BKeni KenizaОценок пока нет
- Abnormal Uterine Bleeding - Surgical ManagementДокумент14 страницAbnormal Uterine Bleeding - Surgical ManagementNikhil DevОценок пока нет
- Factory Program Library List v1.0Документ9 страницFactory Program Library List v1.0Ronaldo DamattaОценок пока нет
- TCNHS - Diagnostic-test-G8-cookery 7&8Документ2 страницыTCNHS - Diagnostic-test-G8-cookery 7&8Elna Grace Dicon-Ybañez100% (4)
- CP Inf4Документ357 страницCP Inf4Rugwed JadhavОценок пока нет
- 9) Expt No - 9 (Halleffect)Документ16 страниц9) Expt No - 9 (Halleffect)Pollack Prittam ChoudhuryОценок пока нет
- Unit 21Документ22 страницыUnit 21Yuni IndahОценок пока нет
- Video Wall, Digital Signage & C'Type Serial NumberДокумент8 страницVideo Wall, Digital Signage & C'Type Serial NumberAbhijit BarmanОценок пока нет
- VisakhapatnamДокумент27 страницVisakhapatnamCherukupalli Gopala KrishnaОценок пока нет
- Antenatally Diagnosed Kidney AnomaliesДокумент17 страницAntenatally Diagnosed Kidney AnomalieslauraОценок пока нет
- CN 235 Aircraft DefinitionДокумент22 страницыCN 235 Aircraft DefinitionMoch Dedy100% (4)
- Obs and Gynae PassmedДокумент7 страницObs and Gynae PassmedrahulОценок пока нет
- Tugas Topic 4 Devi PermatasariДокумент8 страницTugas Topic 4 Devi PermatasariMartinaОценок пока нет
- ELK-3 550 1HC0000742AFEnДокумент20 страницELK-3 550 1HC0000742AFEnOnur FişekОценок пока нет
- COR5500U Series: Digital and CRT Readout OscilloscopeДокумент7 страницCOR5500U Series: Digital and CRT Readout OscilloscopeFlavio FalcãoОценок пока нет
- Esthetics and Shade Communication: A Practical Approach: Clinical ApplicationДокумент21 страницаEsthetics and Shade Communication: A Practical Approach: Clinical Applicationcatalin_adinaОценок пока нет
- Vivo X5Pro Smartphone Specifications: Brand and ModelДокумент4 страницыVivo X5Pro Smartphone Specifications: Brand and ModelEric AndriantoОценок пока нет
- G 62 - 14 PDFДокумент4 страницыG 62 - 14 PDFjose floresОценок пока нет
- Pirastro Extract From Catalogue 2022-05-22Документ72 страницыPirastro Extract From Catalogue 2022-05-22arno8817Оценок пока нет